
Cardiovascular Ergometry and Telemetry in Biomedical Control of Cuban Athlete
Ergometría y telemetría cardiovascular en el control biomédico del deportista cubano
Teresita Duany-Díaz , Cesia Rivera Garmendía, Margiolis Colás Viant
Abstract
Introduction. The digital transformation in health drives the increase of new software, aligned with the dynamics of the development of information and communications technologies (ICTs).
Objective. 1) To justify the benefits of using digital medical technologies -ERGOCID, METALYZER, MOVICORDE and CARDIOTRAINING-CIDC- in the biomedical monitoring of Cuban high-performance athletes. 2) To present the innovations that are carried out in ergometry and field tests during the cardiovascular medical monitoring of Cuban athletes.
Method. Prospective, longitudinal study of innovation and development between January 2018 and December 2023. The universe consisted of 490 athletes from national teams in the different Olympic competition sports. The selective and intentional sample was made up of athletes, both men and women, from combat sports: judo, wrestling, boxing, taekwondo, karate, and fencing. 187 athletes were studied: 101 men and 86 women. The ages of the participants ranged between 17 and 34 years old.
Results. Ergometry-specific protocols were designed, which constitute a technological innovation, for wrestling, judo, boxing, and taekwondo. Telemetric studies were carried out with MOVICORDE during training in taekwondo, karate, and fencing. The CARDIOTRAINING-CIDC software was created and used.
Conclusion. The use of digital technologies has been very beneficial in the medical monitoring and sport performance of athletes. The innovations made, the design of gesture-specific ergometric protocols, and the creation of the VBA CARDIOTRAINING-CIDC macro were very useful in sports biomedical control.
Keywords
Athletic performance; electrocardiography; heart rate; software; sports medicine; wireless technology.
Resumen
Introducción. La transformación digital en salud impulsa el aumento de nuevos softwares, alineada con la dinámica del desarrollo de las tecnologías de la información y las comunicaciones (TICs).
Objetivos. 1) Fundamentar los beneficios de la utilización de las tecnologías médicas digitales -ERGOCID, METALYZER, MOVICORDE y CARDIOTRAINING-CIDC- en el control biomédico de los deportistas de alto rendimiento cubano. 2) Presentar las innovaciones que se realizan en la ergometría y pruebas de terreno durante el seguimiento médico cardiovascular del deportista cubano.
Método. Se realizó un estudio prospectivo, longitudinal, de innovación y desarrollo, entre enero de 2018 y diciembre de 2023. El universo quedó constituido 490 deportistas de los equipos nacionales en los diferentes deportes de competición olímpica. La muestra selectiva e intencional la conformaron los deportistas, tanto hombres como mujeres, de los deportes de combate: judo, lucha, boxeo, taekwondo, kárate y esgrima. Fueron estudiados 187 deportistas; 101 varones y 86 féminas. Las edades de los participantes oscilaron entre 17 y 34 años.
Resultados. Se diseñaron protocolos ergométricos gesto-específicos que constituyen una innovación tecnológica, para lucha, judo, boxeo y taekwondo. Se realizaron estudios telemétricos con MOVICORDE durante el entrenamiento de taekwondo, kárate y esgrima. Fue creado y utilizado el software CARDIOTRAINING-CIDC.
Conclusión. El uso de tecnologías digitales resultó muy beneficioso en el seguimiento médico y del rendimiento atlético de los deportistas. Las innovaciones realizadas, el diseño de protocolos ergométricos gesto-específicos y la creación de la macro VBA CARDIOTRAINING-CIDC resultaron de gran utilidad en el control biomédico deportivo.
Palabras clave
Electrocardiografía; frecuencia cardíaca; medicina deportiva; rendimiento atlético; software; tecnología inalámbrica.
Introduction
Information and communications technologies (ICTs), since their appearance and expansion during the 20th century, have provided new forms of perception and exchange between people. It is a process that has led to the beginning of a new era, which has been called "the information and knowledge society", which sets challenges and opportunities for development in an accelerated manner, as never before in the history of humanity [1]. Technological innovation in educational methods, with its massive and daily application, allows the transformation of content, action, and social thought [2]. The continuous and rapid development of ICTs currently introduces changes in all areas: in the world of work, in education and health systems, production, trade, finance, politics, and human relations. This process involves a cultural change that implicates the whole society, from the individual level to the governmental sphere [3-5].
In the health sector, technology has rapidly conquered the processes of research, diagnosis, and treatment of users of medical services [6]. Within the context of public policies both in Cuba and in the world, the processes of computerization of health systems and services are developed within the framework of the "Global Strategy Project on Digital Health 2020-2025", designed by the World Health Organization [7]. Around this global purpose, elements of digital health, eHealth or cyber health appear, where the application of ICTs in surveillance, prevention, promotion, and health care systems, as well as in education, knowledge, and research become a fundamental pillar [8]. The digital health strategy establishes advanced technologies as determinants of the future of global health [9].
The digital transformation in health stimulates the increase of new technologies of software, aligned with the dynamics of the development of ICTs, as well as the training of qualified professionals and the times that the processes of science and innovation require for the benefit of a better health service [3]. In the processes of clinical diagnosis, medical treatments, and in the prevention of diseases, ICTs have also burst onto the scene in an accelerated manner [2,10]. In Cuba, the different medical specialties opt for the use of digital technologies, with which there has been an increase in quality and efficiency in health services [11].
The Cuban Health System provides detailed attention to the sports population, especially in high-performance athletics. Different specialties such as cardiology, orthopedics and traumatology, psychology and physiotherapy, among many others, come together in the sports field to achieve comprehensive health and better performance of athletes in the largest of the Antilles. The use of ICTs in this environment is a crucial element, since monitoring, usually at a certain distance, of the athlete during his training is part of the objectives to guarantee his sports efficiency, with an optimal state of health [12-15]. It is in this ambit that in the Cardiovascular Area of the Cuban Sports Research Center, digital technological alternatives and innovations are developed such as gesture-specific ergometry, so called because it is performed in the likeness of the particular technical movements of the sport modality, to which is added the use of implements designed to achieve such ergometric objective. Likewise, remote monitoring of heart rate is implemented with the MOVICORDE wireless system during training, and the use of the CARDIOTRAINING-CIDC software, for better use of cardiovascular parameters in the individualization of training plans [16].
Current protocols for sports ergometry are mostly performed on a treadmill or ergometric bicycle. The ergometry test should be performed by simulating the participant's preferred activity to make it as specific and real as possible [17,18]. The measurement of cardiorespiratory capacity through ergospirometry, by using traditional ergometers or current protocols, are still insufficient to satisfy the need for knowledge of the physiological parameters that the medical team, the coach, and the physical trainer need for adequate training planning [19,20]. This calls for a redesign that allows ergometry to be carried out in a way that resembles the sports movements performed in athletics, thus offering effective results comparable to those obtained in training and competition. Ergometry therefore offers greater scientific value for perfecting the individualization of training.
For this reason, this study is conducted with the following objectives: 1) to justify the benefits of using digital medical technologies: ERGOCID, METALYZER, MOVICORDE, and CARDIOTRAINING-CIDC in the biomedical monitoring of high-performance Cuban athletes. 2) To present the innovations being implemented in ergometry and field testing during the cardiovascular medical monitoring of Cuban athletes.
Method
A prospective, longitudinal, innovation, and development study was conducted between January 2018 and December 2023.
The population consisted of 490 athletes, all of them from national teams in the different Olympic competition sports, who attended the Cuban Sports Research Center (Centro de Investigaciones del Deporte Cubano, CIDC for its acronym in Spanish) during the period indicated for performing ergometry, as designated by the sports medical control, as well as those who underwent cardiovascular studies on the training ground.
The selective and intentional sample was made up of athletes from combat sports: judo, wrestling (in its freestyle and Greco-Roman modalities), boxing, taekwondo, karate, and fencing, both men and women, each belonging to the national team. A total of 187 athletes were studied: 101 men and 86 women. Participants ranged in age from 17 to 34 years-old. The selection criteria were based on the sport's greatest impact on medals and international competitive results (Central American, Pan American, World and Olympic events) and on the athletes' current chances of qualifying for upcoming international events in their disciplines.
The following were considered as exclusion criteria: the presence of a contraindication for ergometry or telemetric analysis at the time of the test (acute infectious disease, fever, decompensation of a chronic disease such as high blood pressure or diabetes mellitus, among others) or the individual's refusal to take the test.
It should be noted that all athletes in the chosen sports met the selection criteria, and each agreed to participate voluntarily in the study. The research was approved by the Ethics Committee of the Cuban Sports Research Center on June 25, 2024, under code No. 14/2024.
The judo, boxing, wrestling, and taekwondo athletes performed a gesture-specific ergometric test, while the fencers, karatekas, and taekwondo athletes underwent a cardiovascular telemetry study with the MOVICORDE system on the training ground. Each subject in the study was offered the CARDIOTRAINING-CIDC software for better use of the results in both tests [16,21].
Before each cardiovascular control test (ergometry and telemetry) various aspects were evaluated, as expressed below:
• Anthropometry: Before starting the stress test and telemetry, the following were taken at rest: height (cm), weight (kg).
• Both the ergometric and telemetry tests were performed on the athletes during the same period of sports training: special preparation (this is the stage within the planning of training where the fundamental objective is the acquisition of sports form by increasing the potential of physical qualities with a more concentrated specialization in the athletic modality practiced by the subject) [16,17].
• Prior to the start of the stress test and the field test with telemetry measurement, the purpose and implementation of the test were explained, and voluntary consent to participate in the study was obtained from each of the athletes.
• Heart rate and blood pressure data were recorded at rest, during ergometric effort or training and during recovery.
• In each case, a maximum-intensity warm-up was performed, similar to that which takes place before training or competition, lasting at least 20 minutes. The ergometry test also included a three-minute initial adaptation period to the ergometer, according to the protocol for the sport.
• The heart rate and electrocardiogram were recorded using continuous monitoring with the ERGOCID software during ergometry, and the MOVICORDE during cardiac monitoring on the training ground.
• The predicted maximum heart rate was calculated using the formula: 220 - age, automatically computed by the ergospirometer software (ERGOCID) and manually in the field tests using the MOVICORDE. An ergometric or terrain test was considered submaximal when the value of the calculated percentage of heart rate exceeded 85% without reaching 90%, and a maximum test, when this parameter equaled or exceeded 90%.
• In ergometry, respiratory gas exchange was determined by direct measurement through the use of the METALYZER sensor, to obtain oxygen consumption, expired carbon dioxide and the relationship between these variables.
• The ergometric test ended when the scheduled protocol was completed or at the moment when the athlete reached fatigue, due to tiredness of the lower limbs.
• Telemetry monitoring using the MOVICORDE system concluded when the training scheduled for the day ended.
The term gesture-specific ergospirometry was created by CIDC researchers (technological innovation of the study) to identify a stress test in which the athlete imitates the biomechanical movement or a technique peculiar of the sport practiced. For this, three fundamental aspects were considered:
1. Ergometer to be used. The similarity with the specific sporting gestures of the athletic modality was taken into consideration.
2. Complements or accessories as necessary to guarantee the particular sporting gesture of the modality. Attachments designed by CIDC researchers or existing in the training areas, which allow the biomechanical movements of interest for ergometry to be carried out in each sport.
3. Simulation of competitive times, as appropriate to the singularities of the sport. The ergometers used were: the ERGOCID AT PLUS treadmill or mat and the CONCEPT 2 rowing ergometer.
All the data obtained: heart rate, blood pressure, oxygen consumption, volume of expired carbon dioxide, duration of the ergometry or of the phases during cardiovascular monitoring of training using the MOVICORDE system, among other parameters, were collected in a digital medical record prepared for each athlete and in the clinical record filed in the Cardiovascular Area of the CIDC.
The variables of interest for the research were:
• Maximum heart rate: measured in beats per minute (bpm), taken from the highest value obtained at the end of each test (ergometric and terrain during training).
• Maximum oxygen consumption: highest value of the volume of oxygen, measured in milliliters per kilogram per minute (ml/kg*min-1), indexed according to body weight.
• Metabolic equivalent: represents the proportion by which the metabolism must rise from its basal level in order to meet the physical activity performed. It is expressed in MET (metabolic equivalent of task), where 1 MET is equivalent to 3.5 ml/kg*min-1, a range that corresponds to the resting value of an individual [16-18].
The data were collected in files of the Microsoft Excel 2016 program for Windows. The statistical treatment of the results was carried out through the SPSS program (Statistical Package for Social Sciences), version 25.0. A descriptive statistical analysis was applied to the results with figures of absolute and relative values, with the means and standard deviations of each parameter. The information was summarized in texts and figures.
Results
In the study, gesture-specific protocols were designed, which constitute a technological innovation, for the following sports:
1) Wrestling (Greco-Roman and freestyle). A treadmill was used at a constant low speed of 7 km/h and, if the athlete tolerated it, it was increased to 10 km/h after two minutes in the final stages. Three stages of four minutes each were programmed; the competitive times for this sport were considered. The wrestler was given dumbbells as accessories so that during the ergometric test he could make rotating arm movements, simulating a fight with an opponent (Figure 1).
Figure 1. Fighter in gesture-specific ergometric test on ERGOCID AT PLUS treadmill, with dumbbells in his hands. Cardiovascular area, CIDC.

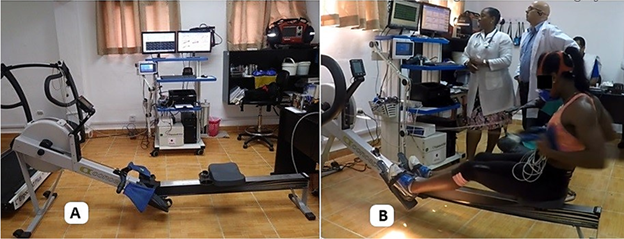
2) Judo. This was performed on a rowing ergometer, to imitate the ne-waza technique or work on the ground; a sleeve and a flap were added to the handlebar of the rowing ergometer, similar to those used with ligaments during training, and which try to emulate the suit or judogi of the opposing judoka, who is gripped with an off-balance technique. The test was divided into three stages of four minutes each, like the competition times in judo (Figure 2).
Figure 2. A: Concept 2 rowing ergometer with sleeve and flap attached to the handlebar for gesture-specific ergometric testing for judo. B: Judoka during ergometry. Cardiovascular area, CIDC.
3) Boxing. This was carried out on a treadmill, with initial speeds of 11 km/h and stage changes every three minutes, with a one-minute break between them, to resemble the times of the rounds in a boxing match. Final speeds of up to 21 km/h were reached, as this is the maximum speed reached by the ERGOCID AT PLUS ergometer (Figure 3).
Figure 3. Gesture-specific ergometric test for boxers on the ERGOCID AT PLUS ergometric mat, with simulation of the times of the rounds in a fight. Cardiovascular area, CIDC.

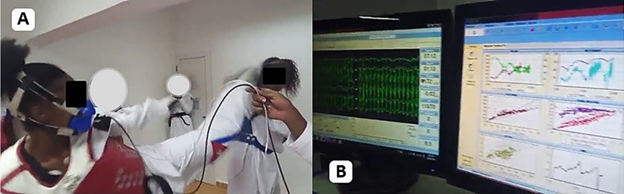
4) Taekwondo. It was carried out on the floor, on a mat, without using an ergometer. It was very novel because the taekwondo athletes simulated a fight with technical movements of both the upper and lower limbs, characteristic of their sport, while the cardiopulmonary parameters were analyzed using the ERGOCID and METALYZER software (Figure 4).
Figure 4. A: Gesture-specific ergometric test for taekwondo athletes, with combat simulation. B: Cardiovascular and respiratory monitoring. Cardiovascular area, CIDC.
The use of ICTs for medical monitoring of athletes was also demonstrated by the use of the MOVICORDE telemetric system. This consists of placing three electrodes on the athlete's chest, connected to a transmitter, which is fastened to the athlete's body by means of a belt before beginning training on the usual sports field. This transmitter emits a signal that reaches a receiving device, connected to a mobile computer by means of a USB cable. This allows the doctor who performs the investigation to observe an electrocardiogram from a distance through the MOVICORDE program installed on the computer, which is why it is known as cardiac telemetry (Figure 5).
Figure 5. MOVICORDE cardiovascular telemetry system. A: Telemetry transmitters and receiver. B: Screenshot of cardiovascular monitoring by telemetry. C: Taekwondo athlete undergoing cardiovascular training monitoring using the MOVICORDE system. Cardiovascular area, CIDC.
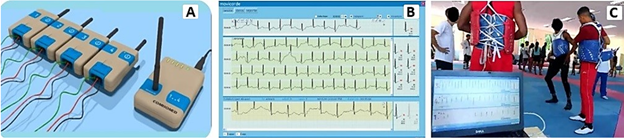
This equipment, manufactured in Cuba, was designed with the objective of monitoring patients with suspected or confirmed heart rhythm disorders, hospitalized or outpatients. This new use was given to athletes, to observe the variations and behavior of heart rate throughout their training.
To support this, CARDIOTRAINING-CIDC, a software created by the authors of this study, was used; it contains a MICROSOFT EXCEL VBA macro, accessible from the computer or mobile device [16,21]. It also consists of an interface that allows entering data such as the full name of the athlete, the date of the test, the age, and the maximum heart rate obtained in the ergometry or during the field test monitored through the MOVICORDE telemetric system (Figure 6).
Figure 6. CARDIOTRAINIG-CIDC software interface, a MICROSOFT EXCEL VBA macro created to calculate training zones based on results in ergometry or cardiovascular telemetric measurement. Cardiovascular area, CIDC.
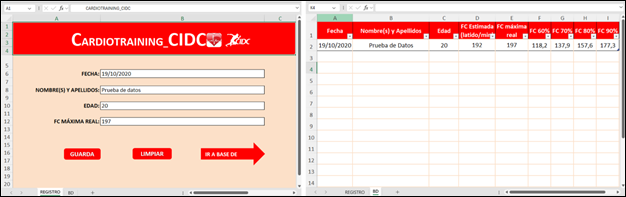
These details, which are entered in sheet 1 of EXCEL (tab "REGISTRO"), will be stored in a database that can be accessed through sheet 2 (tab "BD"). In addition to saving the information entered by the user, it will also show the 60th, 70th, 80th and 90th percentiles of the maximum heart rate.
Discussion
Regarding the stress tests performed on the 18 wrestlers, the average heart rate percentage recorded was 95.7±2.9%. An average maximum oxygen consumption of 53±10.44 ml/kg*min-1 was observed; the metabolic equivalent tolerated in these tests had an average of 15.3±2.5 METS. The values were adequate, and even slightly higher, compared to foreign research carried out by Fierro in 2021 and Flores in 2020, where they studied the cardiovascular physiological parameters of elite wrestlers; it should be noted that wrestling is a sport with a predominantly anaerobic metabolic rate [22,23].
In the ergometric tests performed on the judokas, it was observed that the 25 athletes managed to exceed 90% of the maximum heart rate, with an average of 94.5±3.6%. The average recorded maximum oxygen consumption was 48±11.69 ml/kg*min-1. The tolerated METS presented an average of 14.5±1.9. The results of the ergometric tests carried out on the judokas coincide with the optimal values that appear in similar studies for judo athletes, published by Ouergui (2022) and Franchini (2020), who state that judokas do not need oxygen volumes greater than 40 ml/kg*min-1 to practice this sport, which is a mixed metabolism, with a predominance of anaerobic functions [24,25]. The increase in both heart rate and oxygen consumption was linear and progressive, proportional to the increase in load.
Regarding the ergometries executed to the 32 boxers, the average percentage of maximum heart rate was 98.3±4.2%; the maximum oxygen consumption corresponded to 69±12.54 ml/kg*min-1; the average METs they tolerated was 18.9±2.1. Each of the parameters showed very high results, expected in a mixed sport with an aerobic predominance such as boxing. The data obtained are satisfactory according to the sporting demands of boxers, which require a higher aerobic capacity than other combat sports, as also suggested in studies published between 2020 and 2022 by Ambroży and Venckunas [26,27].
The average percentage of maximum heart rate for the 28 taekwondo athletes was 96.2±7.3%; maximum oxygen consumption averaged 57.5±8.6 ml/kg*min-1, while the average metabolic equivalent was 15.9±3.2 METS. These values also exceeded those reported in a systematic review of studies analyzing cardiovascular variables measured in elite taekwondo athletes, which was presented by Aponte and Segura in 2022 [28], and this responds to the excellent preparation of Cuban athletes and the ability of specific gesture ergometry to achieve maximum levels of effort.
The MOVICORDE telemetric system was used in sports such as taekwondo, applied to 29 of its representatives; in karate, where it was used with 20 athletes and in fencing, applied to 35 of its members (Figure 5), with excellent results. It allowed measuring the progression and recovery of heart rate in the athlete's usual environment during a normal training day. Being a technology that can be used simultaneously with the measurement of up to eight subjects, it was possible to specify, in all cases, the absence of heart rhythm disorders during the training of each athlete. As proposed in their research by authors such as Vega (2020) and Wong (2022), the high impact of computer applications and services in health interventions used for the benefit of athletes was verified [12,13]. Electrocardiographic alterations were ruled out in athletes who appeared to have presyncopal or syncopal symptoms. It helped to assess the physiological capabilities of athletes and to establish signs of overtraining, and was also useful in reorganizing the individual training plan based on data obtained by the MOVICORDE telemetric system; the different ranges of the training zones were calculated in a personalized way from the maximum heart rate obtained.
The CARDIOTRAINING-CIDC software (Figure 6), a Microsoft Excel VBA macro, was created by the authors, so athletes, coaches, doctors, and physical trainers can be guided in a truthful and scientific way regarding the monitoring and evaluation of training. Experts such as Ramírez (2021) and Vidal (2023) suggest that the creation and use of information and communication technologies as a performance factor are strategies that allow reducing the technological gap, on the path of digital transformation in the field of health in its different applications [9,10]. This coincides with what was recorded in this study, where through the use of new software, the percentages derived from the maximum heart rate are obtained, both in ergometry and in field tests. These values represent the ranges of the training zones, to guide individual planning, which is one of the pillars of modern sports preparation. It also allows for comparing, over the weeks following the test, the results with the values of ergometric or field tests that may be performed in subsequent phases, to determine whether the objectives set out in the sports preparation plan are being met.
Limitations and recommendations
Limitations of the research were the performance of fewer ergometries and field tests than expected, because they are expensive procedures with restricted access that prevented a greater number of these processes from being carried out.
Other missing situations were the lack of taking samples for blood lactate analysis, so important in correlation with cardiopulmonary variables, due to the scarcity of this resource during the study.
It is recommended that the scientific community continue to study and research the application of specific gestural ergometric protocols and cardiac monitoring using the MOVICORDE system in each sport, for the benefit of the health and biomedical monitoring of each athlete's training and physical activity practitioner. As a final proposal, the results of this research should be used to improve the Manual of Procedures for Functional and Field Laboratory Testing in Applied Sports Medicine.
Conclusions
• The use of digital technologies such as ERGOCID software for cardiovascular monitoring and METALYZER for the analysis of respiratory variables during ergometry, and the MOVICORDE telemetry system for cardiovascular control in sports training, were very beneficial in the medical and athletic performance monitoring of the high-performance athletes studied.
• The innovations made, the design of gesture-specific ergometric protocols and the creation of the VBA CARDIOTRAINING-CIDC macro, were very useful in biomedical sports control.
References
1. Robledo-Madrid P. Impacto de la aplicación de las Tecnologías de la Información (TICs) en un modelo de atención médica. RSM [Internet]. 2019;73(2):96-104. doi: https://doi.org/10.56443/rsm.v73i2.17
2. Ramos-Delgado A, Vidal-Ledo MJ, Rodríguez-Díaz A, Barthelemy-Aguilar K, Torres- Ávila D. Salud y transformación digital. Educación Médica Superior [Internet]. 2022;36(2):e3442. Available from: https://ems.sld.cu/index.php/ems/article/view/3442
3. León GER. La transformación digital en Cuba: retos para la industria de aplicaciones y servicios informáticos. In: Ruiz-Jhones A, Delgado-Fernández T, Febles-Estrada A, Estévez-Velarde S, editors. Habilitando la Transformación Digital. Tomo II [Internet]. La Habana: Unión de Informáticos de Cuba & Editorial UH; 2022[cited 2025 Jan 2], p. 305-16 Available from: https://repositorio.uci.cu/handle/123456789/10428
4. Belmonte IA, Collado RS, Yuguero O, Oliva JA, Martínez-Millana A, Pérez CS. La alfabetización digital como elemento clave en la transformación digital de las organizaciones en salud. Aten Primaria [Internet]. 2024;56(6):102880. doi: https://doi.org/10.1016/j.aprim.2024.102880
5. Arias-López MP, Ong BA, Borrat-Frigola X, Fernández AL, Hicklent RS, Obeles AJT, et al. Digital literacy as a new determinant of health: A scoping review. PLOS Digit Health [Internet] 2023;2(10):e0000279. doi: https://doi.org/10.1371/journal.pdig.0000279
6. Monasterio-Astobiza A. Medicina digital y el futuro de la salud. Dilemata [Internet]. 2020;(32):5-16. Available from: https://www.dilemata.net/revista/index.php/dilemata/article/view/412000346
7. World Health Organization Team (WHO). Estrategia mundial sobre salud digital. 2020-2025 [Internet]. Geneva: WHO; 2021 [cited 2025 Jan 02]. 50 p. Available from: https://iris.who.int/handle/10665/344249
8. Vialart-Vidal MN, Vidal-Ledo MJ, Sarduy-Domínguez Y, Delgado-Ramos A, Rodríguez- Díaz A, Fleitas-Estévez I, et al. Aplicación de la eSalud en el contexto cubano. Rev Panam Salud Publica [Internet]. 2018;42:e19. doi: https://doi.org/10.26633/RPSP.2018.19
9. Ramírez-Pérez JF, López-Torres VG, Vidal-Ledo MJ, Ramírez-Pérez AR, Morejón- Valdés M. Las tecnologías de la información y la comunicación como factor de desempeño competitivo en instituciones de salud. Rev cuba inf cienc salud [Internet]. 2021;32(2):1-30. Available from: https://acimed.sld.cu/index.php/acimed/article/view/1685
10. Vidal-Alaball J, Alarcón-Belmonte I, Panadés-Zafra R, Escalé-Besa A, Acezat-Oliva J, Saperas-Pérez C. Abordaje de la transformación digital en salud para reducir la brecha digital. Aten Primaria [Internet]. 2023;55(9):102626. doi: https://doi.org/10.1016/j.aprim.2023.102626
11. Ramírez Pérez JF, López Torres VG, Ramírez Pérez AR, Morejón Valdés M. Tecnologías de la Información y la Comunicación en Salud: Análisis de Componentes Principales en la evaluación del desempeño competitivo. Entre Ciencia e Ingeniería [Internet]. 2021;15(30):22-9. doi: https://doi.org/10.31908/19098367.2618
12. Vega-Izaguirre L, López-Cossio F, Ramírez-Pérez JF, Orellana-García A. Impacto de las aplicaciones y servicios informáticos desarrollados por la Universidad de las Ciencias Informáticas para el sector de la salud. RCIM [Internet]. 2020;12(1):58-75. Available from: http://scielo.sld.cu/scielo.php?script=sci_arttext&pid=S1684-18592020000100058&lng=es&tlng=es
13. Wong HTH, Prankumar SK, Cui J, Tumwine C, Addo IY, Kan W, Noor MN. Information and communication technology-based health interventions for transgender people: A scoping review. PLOS Glob Pub Health [Internet]. 2022;2(9):e0001054. doi: https://doi.org/10.1371/journal.pgph.0001054
14. Yogesh MJ, Karthikeyan J. Health Informatics: Engaging Modern Healthcare Units: A Brief Overview. Front Public Health [Internet]. 2022;10:854688. doi: https://doi.org/10.3389/fpubh.2022.854688
15. Duany-Díaz TD, Colás-Viant M. Consideraciones médicas entorno a la reincorporación deportiva después de la COVID-19. Rev cubana med [Internet]. 2021:60(1):e1645. Available from: https://revmedicina.sld.cu/index.php/med/article/view/1645
16. Duany-Díaz TD. Ergometría para boxeadores y Cardiotraining_CIDC en la era post COVID-19. RICCAFD [Internet]. 2022;11(2):77-89. doi: https://doi.org/10.24310/riccafd.2022.v11i2.14654
17. Duany-Díaz T, Colás-Viant M, Padrón-Pérez AJ. Ergometría cardiopulmonar gesto específico para judocas élites. RICCAFD [Internet]. 2023;12(3):168-82. doi: https://doi.org/10.24310/riccafd.12.3.2023.17443
18. Araujo-Rivas MA, Hernández-Guerrero AJ. Parámetros morfo-funcionales básicos del rendimiento atlético evaluados en los deportes. Lect educ fís deportes (B. Aires) [Internet]. 2021;25(273):175-90. doi: https://doi.org/10.46642/efd.v25i273.1645
19. Mazaheri R, Schmied C, Niederseer D, Guazzi M. Cardiopulmonary Exercise Test Parameters in Athletic Population: A Review. J Clin Med [Internet]. 2021;10(21):5073. doi: https://doi.org/10.3390/jcm10215073
20. Duany-Díaz TD. Determinación ergométrica del índice de eficiencia miocárdica en atletas élites cubanos. Rev Cubana Inv Bioméd [Internet]. 2023;42(1):e2516. Available from: https://revibiomedica.sld.cu/index.php/ibi/article/view/2516
21. Duany-Díaz TD, Colás-Viant M. Control cardiovascular en el entrenamiento deportivo mediante ergometría y empleo del software Cardiotraining_CIDC. Rev Cubana Inv Bioméd [Internet]. 2023;42(1):e1664. Available from: https://revibiomedica.sld.cu/index.php/ibi/article/view/1664
22. Fierro-Subía KE. Condición aeróbica y su relación con fuerza explosiva y flexibilidad en deportistas de lucha olímpica de la Federación Deportiva de Imbabura, periodo 2020-2021 [dissertation]. Ibarra: Universidad Técnica del Norte; 2021. 90 p. Available from: http://repositorio.utn.edu.ec/handle/123456789/11188
23. Flores FJ, Carballido LG, Cagigas EV. Estudio de indicadores fisiológicos y psicológicos en luchadores del estilo libre. Rev Cub Med Dep & Cult Fis [Internet]. 2014;9(2). Available from: https://revmedep.sld.cu/index.php/medep/article/view/177
24. Ouergui I, Delleli S, Chtourou H, Formenti D, Bouhlel E, Ardigò LP, et al. The Role of Competition Area and Training Type on Physiological Responses and Perceived Exertion in Female Judo Athletes. Int J Environ Res Public Health [Internet]. 2022;19(6):3457. doi: https://doi.org/10.3390/ijerph19063457
25. Franchini E, Dunn E, Takito MY. Reliability and Usefulness of Time-Motion and Physiological Responses in Simulated Judo Matches. J Strength Cond Res [Internet]. 2020;34(9):2557-64. doi: https://doi.org/10.1519/JSC.0000000000002727
26. Ambroży T, Maciejczyk M, Klimek AT, Wiecha S, Stanula A, Snopkowski P, et al. The Effects of Intermittent Hypoxic Training on Anaerobic and Aerobic Power in Boxers. Int J Environ Res Public Health [Internet]. 2020;17(24):9361. doi: https://doi.org/10.3390/ijerph17249361
27. Venckunas T, Bruzas V, Stasiulis A, Snieckus A, Mockus P, Kamandulis S. Cardiorespiratory Responses to Specific and Nonspecific Exercise in High-Profile Amateur Boxers. J Strength Cond Res [Internet]. 2022;36(3):717-22. doi: https://doi.org/10.1519/jsc.0000000000003496
28. Aponte-Cáceres JA, Segura-Caicedo DE. Valoración de la potencia anaeróbica en taekwondo. Una revisión sistemática. Rev Act Fis & Dep [Internet]. 2022;8(1). doi: https://doi.org/10.31910/rdafd.v8.n1.2022.1967