
Do Older Adults Engaged in a Community-Based Exercise Program Have Better Mental Health Indicators? A Static Group Comparison Study in a Brazilian Regional Area
¿Tienen los adultos mayores que participan en un programa de ejercicio basado en la comunidad mejores indicadores de salud mental? Un estudio comparativo de grupos estáticos en un área regional brasileña
Matheus Vitor Beserra Cavalcanti, Paula Ferreira Mendes do Nascimento, Leonardo dos Santos Oliveira
Abstract
Introduction. The evidence on the effectiveness of community-based exercise program (CBEP) on psychological distress among older adults appears unclear, especially in developing countries.
Objective. To compare the mental health of older adults engaged in an 8-week CBEP with a physically inactive control group living in a Brazilian regional area.
Method. In a static group comparison design (a single post-exposure measure), older adult women engaged in a community-based exercise program [CBEP, n = 24, mean (SD), age: 67 (9) years, BMI: 27.7 (5.1) kg/m2] and a physically inactive control group [PIC, n = 30, mean (SD), age: 69 (6) years, BMI: 29.5 (3.4) kg/m2] participated of this study. The CBEP was conducted 3x/wk for 8 weeks, with Pilates activities (90 min/wk), water-aerobic exercises (90 min/wk) and Brazilian capoeira (120 min/wk). Self-report data on sociodemographic, clinical characteristics and indicators of stress, anxiety and depression (DASS-21 scale) were assessed to provide a posttest to both the experimental group and the comparison group.
Results. The Welch ANOVA showed lower levels of anxiety (Cohen’s d = 2.9), depression (Cohen’s d = 4.2) and stress (Cohen’s d = 3.5) in the CBEP group compared to the PIC group (P<0.001). Likewise, the psychological distress was statistically lower for the CBEP group (Cohen’s d = 3.9, P<0.001).
Conclusion. Compared to their physically inactive counterparts, female older adults who participate in a CBEP have the best mental health indicators.
Keywords
Anxiety; depression; elderly; physical activity; community health services.
Resumen
Introducción. La evidencia sobre la efectividad del programa de ejercicio basado en la comunidad (CBEP por sus siglas en inglés) sobre el malestar psicológico entre los adultos mayores parece poco clara, especialmente en los países en desarrollo.
Objetivo. Comparar la salud mental de adultos mayores que participan en un CBEP de 8 semanas con un grupo de control físicamente inactivo que vive en un área regional brasileña.
Método. En un diseño de comparación de grupos estáticos (una única medida posterior a la exposición), mujeres adultas mayores que han realizado en un programa de ejercicios comunitario [CBEP, n = 24, media (DE), edad: 67 (9) años, IMC: 27,7 (5,1) kg/m2] y un grupo de control físicamente inactivo [PIC, n = 30, media (DE), edad: 69 (6) años, IMC: 29,5 (3,4) kg/m2] participaron en este estudio. El CBEP se realizó 3 veces por semana durante 8 semanas, con actividades de Pilates (90 min/semana), ejercicios aeróbicos acuáticos (90 min/semana) y capoeira brasileña (120 min/semana). Se evaluaron datos de autoinforme sobre características sociodemográficas, clínicas e indicadores de estrés, ansiedad y depresión (escala DASS-21) para proporcionar una prueba posterior tanto al grupo experimental como al grupo de comparación.
Resultados. El ANOVA de Welch mostró niveles más bajos de ansiedad (d de Cohen = 2,9), depresión (d de Cohen = 4,2) y estrés (d de Cohen = 3,5) en el grupo CBEP en comparación con el grupo PIC (P<0,001). Asimismo, el distrés psicológico fue estadísticamente menor para el grupo CBEP (d de Cohen= 3,9; P<0,001).
Conclusión. En comparación con sus homólogos físicamente inactivos, las mujeres mayores que participan en un CBEP presentan los mejores indicadores de salud mental.
Palabras clave
Ansiedad; depresión; anciano; actividad física; servicios de salud comunitaria.
Introduction
In the contemporary era, physical activity (PA) is fundamental to healthy aging [1,2]. A substantial body of research has documented the deleterious impact of functional decline associated with aging on mental health (MH), which increases the risk of depression and anxiety disorders [3,4]. Now more than ever, a considerable number of chronic diseases, including mental disorders, have been observed in older adults, either as a consequence of insufficient PA or increased sedentary behavior [2,5]. In this regard, a variety of PA approaches have been proposed with the objective of mitigating the adverse effects of aging and providing comprehensive care for the MH of the elderly population [2,6].
A notable approach that has gained prominence in public health strategies is the community-based exercise program (CBEP). These interventions are widely recognized as a top public health priority on a global scale. In general, this model provides accessible and inclusive opportunities for regular PA in groups under professional supervision, typically in public spaces, whether indoor or outdoor [7,8]. Moreover, these programs are effective in promoting long-term adherence to PA and enhancing social connections and support [9-11]. Prior research has demonstrated that CBEPs can positively impact health outcomes [11-16]. Consequently, the CBEPs would provide a comprehensive approach to improving the MH for older adults.
Recent systematic reviews have suggested that exercise programs are effective in improving lower limb strength and function [12], and increasing/maintaining physical performance [15] in community-dwelling older adults. For instance, a 6-month exercise program has been shown to reduce fatigue levels and salivary cortisol in community-dwelling older adults [17]. However, the implementation of CBEPs has been restricted to conventional modalities, including walking, resistance exercises, balance exercises, and calisthenics [7,11]. Furthermore, the efficacy of CBEPs in addressing psychological distress among older adults appears to be constrained, particularly in developing countries [7,11].
In Brazil, the implementation of policies and programs has facilitated increased engagement in PA among the elderly population [18-20]. The majority of initiatives aimed at promoting PA in the country are implemented through CBEPs (e.g., “Health Academy Program”, “City Academy Program”) and public institutions (e.g., Social Assistance Reference Center - “CRAS”) [19-21]. Nonetheless, it is fundamental to recognize that CBEPs may exhibit variability due to the flexibility of Brazilian public policies and in response to the unique challenges of PA in different geographic regions (e.g., climate, cultural and sociodemographic diversity) [18-21]. Given the broad scope of PA initiatives, there is a paucity of research examining CBEPs within the nation.
Understanding the factors associated with the potential psychosocial benefits of CBEP is an important public health focus, particularly when these programs are offered in non-metropolitan areas [7]. In light of the aforementioned considerations, the objective of this study is to compare the MH of older adults engaged in an 8-week CBEP with a physically inactive control group living in a Brazilian regional area. It is hypothesized that the CBEP group would have the best MH indicators, including stress, anxiety, and depression, among the elderly population. The findings of this study are expected to contribute to the development of best practices for CBEPs and assist public health services in promoting MH for this age group in regional settings.
Method
Study design and ethics
The present study employs a pre-experimental design with a static group comparison [22]. Following the administration of the treatment, a comparison group was selected, and a posttest was performed to both the experimental group and the comparison group [22]. Consequently, a single post-exposure assessment of the MH was conducted in the exercise (CBEP) and physically inactive control (PIC) groups. The research was conducted in Guarabira, a city in the state of Paraíba, Brazil (located in the Northeast region of the country). According to the Brazilian Institute of Geography and Statistics (IBGE for its acronym in Spanish) [23], Guarabira has a demographic density of 353.99 inhabitants/km² and 57,484 inhabitants in the last census (data from 2022). The records also indicate a human development index (HDI) of 0.673 (data from 2010). The dimensions that contributed the most to the index were life expectancy (0.812), followed by per capita income (0.641), and education (0.586).
Participants
All participants of CBEP group were residents of Guarabira who were recruited in the social program at a CRAS (n = 29). The participant inclusion criteria were as follows: a) men and women aged between 65 and 79, b) literate, and c) older adults who do not have decompensated diabetes or hypertension. Exclusion criteria included: a) older adults who did not complete 80% of the CBEP sessions (n = 0), or b) those who were engaged in cognitive or drug therapy for mental disorders or any other type of vigorous PA or competitive sports during the data collection during the study (n = 5). After the treatment, the PIC group (n = 30) was recruited through word-of-mouth communication and social media [24].This group consisted of older women who had not engaged in regular PA in the previous 8 weeks. The non-probability sampling method was employed due to the geographic availability of the participants.
The study was approved by the local ethics committee (protocol CAAE: 68161023.2.0000.5188) in accordance with the ethical standards set forth by the Declaration of Helsinki and National Health Council.
Procedures
The data collection process entailed the administration of a retrospective self-administered form between May 2023 and June 2023. The estimated time required to complete the form was approximately 20 minutes, and it was comprised of two sections: sociodemographic characteristics and clinical aspects, and mental health assessment. The data collection process occurred during the morning hours (7:00-10:00 a.m.) in a private setting, with the presence of a trained researcher who was not involved in the CBEP.
Measures
A set of self-reported data was collected, encompassing demographic and health-related characteristics such as sex, age (years), height (m), body mass (kg), level of education (incomplete high school or complete high school), medication use or cognitive therapy for mental disorders (yes/no), and pre-existing medical conditions. Moreover, the Brazilian short version of the International Physical Activity Questionnaire (IPAQ) was used to assess self-reported PA [25]. The IPAQ assesses the frequency (in days) and time spent performing moderate to vigorous PA, walking, and sitting in bouts of at least 10 min over the previous 7 days.
The assessment of indicators of stress, anxiety, and depression was conducted using the Brazilian version of Depression Anxiety and Stress Scale (DASS-21) [26]. This instrument has adequate internal consistency for the anxiety (α= 0.86), depression (α= 0.92) and stress (α= 0.90) scales [27]. The DASS-21 comprises 21 questions, with each subscale consisting of seven items that assess emotional states of depression, anxiety and stress over the last week: anxiety [Q2, Q4, Q7, Q9, Q15, Q19 and Q20], depression [Q3, Q5, Q10, Q13, Q16, Q17 and Q21] and stress [Q1, Q6, Q8, Q11, Q12, Q14 and Q18]. The responses are scored on a Likert four-point scale (0, 1, 2 and 3), ranging from 0 (“Strongly disagree”) to 3 (“Totally agree”) scales [27]. The final DASS-21 score is then calculated by multiplying the raw score by two to interpret the severity indices. Furthermore, the total scores from the depression, anxiety, and stress subscales were aggregated to derive a psychological distress index, which serves as a general indicator of MH.
Community-based exercise program (CBEP)
CBEP protocol was administered thrice weekly for a period of eight weeks. The program encompassed a series of activities including Pilates (90 minutes on Tuesdays, afternoons), water-aerobic exercises (90 minutes on Wednesdays, mornings) and Brazilian capoeira (120 minutes on Thursdays, afternoons) were performed. This program was supervised by a Physical Education professional. The exercise sessions comprised a 10-minute dynamic warm-up period, which included joint mobility, stretching exercises, and fast walking; ~30-120 min of Pilates, water-aerobic exercises, or capoeira; and a 10-minute cool-down period. The exercise intensity was not controlled during these sessions.
The Pilates exercises were designed to enhance the strength of the hips and trunk muscles, improve postural balance, and promote stretching of the hips and trunk muscles. The fundamental technique employed was mat Pilates, which involved the use of ball and foam rollers. Each exercise was performed in sets of 8 to 10 repetitions.
The water-aerobic exercises were conducted in a pool with a temperature ranging from 28 to 31°C and a depth of 1.40 to 1.70 meters (all exercises were performed in water depth near the xiphoid process). The sessions were continuous and comprised a series of exercises encompassing flexion, extension, abduction, and adduction of the upper and lower limbs. The exercises also included a twist (trunk rotation). Each exercise was performed in sets of 10 to 20 repetitions.
The capoeira activity entailed a series of agile and complex movements, in which the elderly utilized their feet and hands in conjunction with a variety of “gymnastic-acrobatic” elements. The practice of capoeira was embedded within the context of a ritualized circle, wherein the music served as a conduit for fostering a sense of connection among participants, who engaged in singing and clapping [28]. The absence of codified regulations in capoeira engenders a considerable degree of flexibility in performance. Despite the competitive nature of the modality, older adults do not necessarily prioritize outperforming others through the demonstration of acrobatic, aesthetic, or martial techniques [29].
Data analysis
Data from the categorical variables were presented by absolute (n) and relative (%) frequency. The Chi-square test for heterogeneity was applied to compare the groups. Mean, median, standard deviation (SD), interquartile range (IQR), and 95% confidence interval (95%CI) were used for descriptive analysis of the quantitative variables. Welch ANOVA with bootstrap procedure (n = 1000 samples) was used to analyze the CBEP effect on MH. As an alternative model, an ANCOVA model adjusted for level of education, drugs, and cognitive therapy was also performed. The effect size was calculated by Cohen’s d and interpreted as: d< 0.20 trivial, d = 0.20-0.59 small, d = 0.60-1.19 moderate, d = 1.20-1.99 large, d = 2.00-3.99 very large and d≥ 4.0 almost. Moreover, a posteriori power calculation was performed by the G*Power 3.1.9 (Frans Faul, Germany). The statistical analysis was performed using the IBM Statistical Package for the Social Sciences (SPSS), version 29.0 (IBM Corp., Armonk, USA). A P-value less than 5% was considered statistically significant.
Results
With regard to anthropometric characteristics, the two groups were found to be similar, with the exception of body mass, which was found to be lower in the CBEP group (P = 0.006, Table 1). The CBEP group demonstrated a lower level of education, while the proportion of drug and cognitive therapies was higher in the PIC group (P<0.05, Table 1).
Table 1. Anthropometric and sociodemographic characteristics of older adult women participating in the community-based exercise program (CBEP) and physically inactive control group (PIC).
| Variable | CBEP (n = 24) | PIC (n = 30) | P |
|---|---|---|---|
| Age (years) | 67 (9) | 69 (6) | 0.687 |
| Heigth (m) | 1.5 (0.1) | 1.5 (0.1) | 0.856 |
| Body mass (kg) | 62 (6) | 67 (7) | 0.006 |
| Body mass index (kg/m2) | 27.7 (5.1) | 29.5 (3.4) | 0.134 |
| MVPA (min/wk)* | 240 (210) | 0 (60) | 0.001 |
| Level of education (n, %) | 0.001 | ||
| Incomplete high school | 22 (91.6) | 19 (63.3) | |
| Complete high school | 2 (8.4) | 11 (36.7) | |
| Skin color (n, %) | 0.028 | ||
| White | 6 (25.0) | 1 (3.3) | |
| Brown/Black | 18 (75.0) | 29 (96.7) | |
| Drugs therapy (n, %) | <0.001 | ||
| No | 24 (100.0) | 14 (46.7) | |
| Yes | 0 (0.0) | 16 (53.3) | |
| Cognitive therapy (n, %) | <0.001 | ||
| No | 24 (100.0) | 14 (46.7) | |
| Yes | 0 (0.0) | 16 (53.3) |
Note. Numeric data are reported by mean (SD). MVPA, moderate to vigorous physical activity. *Data presented by median (IQR). Categoric data presented by absolute (n) and relative (%) frequency. P-value for independent t test and qui-square test for numeric and categoric variables, respectively.
The adjusted ANOVA model for the variables of level of education, drugs, and cognitive therapy yielded identical results. Thus, we reported only unadjusted model. The CBEP group had lower levels of anxiety, depression and stress than the PIC group (P<0.05, Table 2). In addition, the psychological distress was statistically lower for the CBEP group (Figure 1). A posteriori calculation demonstrated that this sample had a power ≥80% for detecting ES greater than or equal to 2.0 as significant.
Table 2. Analysis of anxiety, depression and stress indices among older adult women participating in community-based exercise program (CBEP) vs. physically inactive control group (PIC).
| Variable | CBEP (n = 24) | PIC (n = 30) | FWelch | P | ES |
|---|---|---|---|---|---|
| Anxiety | 15.8 [13.0-18.5] | 30.0 [29.1-31.1] | 97.3 | <0.001 | 2.98 |
| Depression | 13.8 [11.2-16.5] | 33.3 [32.2-34.5] | 198.1 | <0.001 | 4.20 |
| Stress | 15.6 [12.9-18.3] | 31.8 [30.9-32.7] | 137.3 | <0.001 | 3.53 |
Note. DAAS-21 scores are presented by mean [95%CI] estimated by Welch's ANOVA with bootstrap procedure. ES, effect size (Cohen's d).
Figure 1. Analysis of the psychological distress (general indicator of mental health) among older adult women participating in the community-based exercise program (CBEP, n= 24) vs. physically inactive control group (PIC, n= 30).
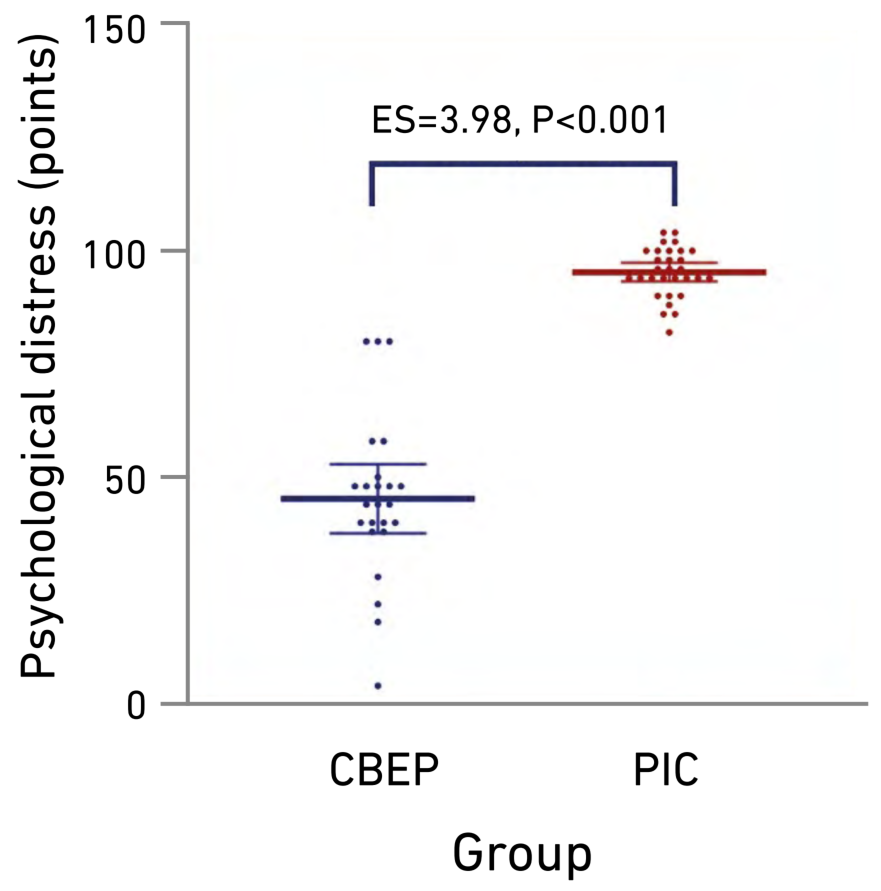
Note. Data are presented by mean (CI95%). F Welch= 171.2, P<0.001. ES, effect size (Cohen’s d).
Discussion
This study compared the MH of older adult women engaged in an 8-week CBEP with a PIC group living in a Brazilian regional area. Our findings support the hypothesis that the CBEP group would have the best MH indicators in older women living in a Brazilian regional area. A seminal aspect of the study was the examination of MH in older participants outside of the south axis of Brazil. Furthermore, the CBEP employed unconventional forms of PA, a strategy that is particularly innovative within the Brazilian context.
Aging is associated with functional decline, which has deleterious effects on a range of outcomes in MH [3,4]. Furthermore, numerous elderly Brazilians continue to experience psychological distress due to the ongoing effects of the pandemic, which has led to an increase in demand for MH services [30]. In this context, an interesting alternative is to offer CBEPs through health centers. Such initiatives have been observed to promote more suitable behaviors, thereby enhancing the health and overall quality of life for the beneficiaries [7,11]. This emphasizes the importance of making CBEPs accessible as part of regional health policies to enable broader participation and promote long-term improvements in the MH of older adults.
CBEPs are low-cost, low-risk, non-invasive, and play a potentially important role in mitigating the decline in functional and psychosocial outcomes common to advancing age [7,9,12]. These programs offer a multifaceted approach to improving MH by providing structured PA combined with social interaction and support [10,11]. Moreover, community-based approaches to PA can reach large numbers of people, often leading to greater improvements and sustainability over time [9]. Thus, CBEPs have the potential to be especially beneficial for individuals facing challenges related to MH, as they provide a comprehensive strategy for enhancing emotional support, motivation from group dynamics, and reduced loneliness [11,31].
A substantial proportion of CBEPs administered to older adults have incorporated conventional modalities, encompassing resistance exercises, aerobic/balance exercises, and calisthenics [7,11-15]. Nonetheless, there is an absence of substantial reporting on psychosocial outcomes in the study results [7,11]. A previous investigation found that endurance exercise training performed 3 hours per week for 12 weeks remained significantly associated with stable or improved cognitive status [14]. A subsequent study demonstrated that a 30-minute exercise period once a week for 12 weeks improved instrumental self-maintenance, intellectual activity and social role [13]. Accordingly, our findings suggest that unconventional forms of PA (e.g., Pilates, capoeira) provided by public services may also have a significant impact on MH.
In Brazil, the promotion of PA represents a fundamental objective within the broader context of health system initiatives designed to enhance population health [18]. In this scenario, local community PA programs have provided a diverse range of activities with a beneficial impact on users' health indicators and contribute to an increase in leisure-time PA [19,20]. Some evidence support that community-based PA interventions reduced depressive symptoms, decreased anxiety, and improved MH functioning in MH service users [11]. Therefore, it can be suggested that public health services in Brazil should consider expanding these initiatives to serve a larger number of older people, including those with MH problems [10,32].
An analysis of relevant sociodemographic factors reveals a noteworthy observation in our study. Despite the higher level of education exhibited by the PIC group, the majority of its members were engaged in pharmacological and cognitive therapies. Furthermore, a greater proportion of individuals with darker skin tones is observed within the PIC group. This may be indicative of worse MH outcomes due to factors such as discrimination and social perception [33]. Therefore, the presence of psychological distress in PIC group, as indicated by these findings, may have contributed to the observed high effect sizes in favor of CBEP.
As demonstrated in the extant literature, the Pilates method has been shown to offer physical and mental benefits [34,35]. A distinguishing aspect of Pilates is its emphasis on mental focus during execution, which has been shown to mitigate stress, fear, and panic in response to anxiety attacks [36,37]. This heightened focus on the present moment may, in turn, foster increased self-confidence and a more positive self-perception, thereby contributing to an enhanced overall sense of mental well-being. In this way, the Pilates method can be regarded as a crucial component in the reduction of stress and anxiety levels, as suggested by the results of this study.
A growing body of research has demonstrated a positive correlation between regular water-aerobic exercises and improved mood, as well as reduced anxiety [38-40]. This practice may create an atmosphere that reduces the perception of physical exertion, and helps promote calm and well-being [38,40]. In addition, group PA programs facilitate an increase in social interaction among participants, thereby establishing a support system among them [10,32,41,42]. Thus, the water-aerobic exercises in CBEP group would play a fundamental role in the interpersonal connections and psychological support. From this perspective, this modality can be recommended as a therapeutic aid for the elderly, with the objective of reducing anxiety levels in practitioners diagnosed with anxiety and depression disorders [38,43].
A series of studies have shown that the practice of capoeira improves both aspects of health-related physical fitness (e.g., muscle strength, flexibility, metabolic parameters) [44,45] and factors related to emotional skills [29,45]. Its practice appears to enhance cognitive performance by expanding the neural pathways of the nervous system as individuals contemplate the intricacies of a particular movement [44,46]. In turn, the social interaction inherent in the practice of capoeira fosters a sense of community and belonging, which may be especially beneficial for MH [28,45,47]. Therefore, this form of PA integrates elements that have the potential to enhance the mental well-being of the elderly in CBEPs.
Notwithstanding the inherent limitations of the study, the findings suggest some practical applications. Initially, programs such as CBEP can be replicated in CRAS or other community centers for the elderly, even with limited resources. The study's findings, even when considering non-probabilistic selection methods, are indicative of the effectiveness of the intervention for specific groups, which may be useful in developing targeted interventions or campaigns. Moreover, the study can serve as a model for community program managers and health policymakers seeking to justify the allocation of resources to PA initiatives for the elderly. This can also help prioritize regions with lower human development indexes, such as Guarabira-PB.
Limitations and Recommendations
Despite the restriction of participation to individuals engaged in cognitive and drug therapies or other forms of PA -as outlined by specific eligibility criteria-, the experimental design does not permit the establishment of direct causality, even with a statistical adjustment. A further consideration was that the participants had been selected prior to the initiation of the study (selection bias), with elderly women enrolled in an existing community program. Moreover, the majority of individuals in the control group were receiving treatment for a mental disorder (psychotherapy or drugs), which may have contributed to the pronounced effect sizes observed. In this study, the absence of randomization may have introduced selection bias, while the lack of blinding could have influenced the perceptions and behaviors of participants and evaluators, thereby potentially impacting the outcomes.
For those who do not regularly engage in PA, as defined in this study as the PIC group, it is recommended that interventions be initiated as soon as possible to mitigate the levels of anxiety, depression, and stress observed. In addition to its role in preventing chronic diseases, maintaining independence and social ties, and reducing isolation, community PA can contribute to the MH of the elderly population [11,13]. It can be reasonably argued that the implementation of PAs in community centers (e.g., CRAS) has the potential to positively impact the overall health and well-being of individuals, which is a significant contributing factor to anxiety and depression. In order to obtain controlled effects of CBEPs, further studies must be conducted with true experimental designs.
Conclusions
Compared to their physically inactive counterparts, female older adults who participate in a CBEP have the best mental health indicators. Public health services may promote psychosocial benefits implementing unconventional forms of PA to motivate this age group in settings identified as regional.
References
1. Dogra S, Dunstan DW, Sugiyama T, Stathi A, Gardiner PA, Owen N. Active aging and public health: Evidence, implications, and opportunities. Annu Rev Public Health [Internet]. 2022;43:439-59. doi: https://doi.org/10.1146/annurev-publhealth-052620-091107
2. Zager Kocjan G, Avsec A, Kavčič T. Feeling too low to be active: Physical inactivity mediates the relationship between mental and physical health. Soc Sci Med [Internet]. 2024;341:116546. doi: https://doi.org/10.1016/j.socscimed.2023.116546
3. Segal DL, Qualls SH, Smyer MA. Aging and mental health. 3rd ed. Hoboken: Wiley-Blackwell; 2018. 480 p.
4. Henríquez J, Henríquez W, Méndez Muñoz R, Ibinarriaga T, Mabe-Castro D, Mabe-Castro M, et al. Cognitive impairment and anxiety in older adults: Characterizations in a high southern latitude population. Rev Investig Innov Cienc Salud [Internet]. 2025;7(1):1-11. doi: https://doi.org/10.46634/riics.326
5. Dempsey PC, Friedenreich CM, Leitzmann MF, Buman MP, Lambert E, Willumsen J, et al. Global public health guidelines on physical activity and sedentary behavior for people living with chronic conditions: A call to action. J Phys Act Health [Internet]. 2021;18(1):76-85. doi: https://doi.org/10.1123/jpah.2020-0525
6. Nascimento PFM, Silva RS, Rodrigues Neto G, Oliveira LS. Treinamento multicomponente e de força melhoram saúde mental e qualidade de vida de idosos. EFDeportes [Internet]. 2024;29(311):71-82. doi: https://doi.org/10.46642/efd.v29i311.7460
7. Fien S, Linton C, Mitchell JS, Wadsworth DP, Szabo H, Askew CD, et al. Characteristics of community-based exercise programs for community-dwelling older adults in rural/regional areas: A scoping review. Aging Clin Exp Res [Internet]. 2022;34(7):1511-28. doi: https://doi.org/10.1007/s40520-022-02079-y
8. Baker PR, Francis DP, Soares J, Weightman AL, Foster C. Community wide interventions for increasing physical activity. Cochrane Database Syst Rev [Internet]. 2015;1(1):Cd008366. doi: https://doi.org/10.1002/14651858.CD008366.pub3
9. Bopp M, Fallon E. Community-based interventions to promote increased physical activity: A primer. Appl Health Econ Health Policy [Internet]. 2008;6(4):173-87. doi: https://doi.org/10.1007/bf03256132
10. Quirk H, Crank H, Harrop D, Hock E, Copeland R. Understanding the experience of initiating community-based physical activity and social support by people with serious mental illness: A systematic review using a meta-ethnographic approach. Syst Rev [Internet]. 2017;6:214. doi: https://doi.org/10.1186/s13643-017-0596-2
11. Tweed LM, Rogers EN, Kinnafick FE. Literature on peer-based community physical activity programmes for mental health service users: A scoping review. Health Psychol Rev [Internet]. 2021;15(2):287-313. doi: https://doi.org/10.1080/17437199.2020.1715812
12. Lim H, Jani NDB, Pang WT, Lim ECW. Community-based exercises improve health status in pre-frail older adults: A systematic review with meta-analysis. BMC Geriatr [Internet]. 2024;24(1):589. doi: https://doi.org/10.1186/s12877-024-05150-7
13. Maki Y, Ura C, Yamaguchi T, Murai T, Isahai M, Kaiho A, et al. Effects of intervention using a community-based walking program for prevention of mental decline: A randomized controlled trial. J Am Geriatr Soc [Internet]. 2012;60(3):505-10. doi: https://doi.org/10.1111/j.1532-5415.2011.03838.x
14. Muscari A, Giannoni C, Pierpaoli L, Berzigotti A, Maietta P, Foschi E, et al. Chronic endurance exercise training prevents aging-related cognitive decline in healthy older adults: a randomized controlled trial. Int J Geriatr Psychiatry [Internet]. 2010;25(10):1055-64. doi: https://doi.org/10.1002/gps.2462
15. Flores-Bello C, Correa-Muñoz E, Sánchez-Rodríguez MA, Mendoza-Núñez VM. Effect of exercise programs on physical performance in community-dwelling older adults with and without frailty: Systematic review and meta-analysis. Geriatrics [Internet]. 2024;9(1):1-18. doi: https://doi.org/10.3390/geriatrics9010008
16. Teixeira do Amaral V, Fernandes B, Ngomane AY, Marçal IR, Zanini GS, Ciolac EG. Short-term community-based exercise programs in low-income older women: Does exercise intensity and modality matters? Exp Gerontol [Internet]. 2021;156:111591. doi: https://doi.org/10.1016/j.exger.2021.111591
17. Tada A. Psychological effects of exercise on community-dwelling older adults. Clin Interv Aging [Internet]. 2018;13:271-6. doi: https://doi.org/10.2147/CIA.S152939
18. Anexo I. Política Nacional de Promoção da Saúde (PNPS). Portaria de ConsolidaÇÃO nº 2, de 28 de Setembro de 2017. Diário Oficial da União (Oct 3, 2017). Available from: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2017/prc0002_03_10_2017.html#ANEXOI
19. Silva AG, Guerreiro CS, Malta DC. Meta‐evaluation of studies on community physical activity programs in Brazil. Int J Health Plann Manage [Internet]. 2023;38(1):252-64. doi: https://doi.org/10.1002/hpm.3585
20. Silva AG, Prates EJS, Malta DC. Evaluation of community physical activity programs in Brazil: A scoping review. Cad Saude Publica [Internet]. 2021;37(5):e00277820. doi: https://doi.org/10.1590/0102-311X00277820
21. Becker L, Gonçalves P, Reis R. Programas de promoção da atividade física no Sistema Único de Saúde brasileiro: Revisão sistemática. Revista Brasileira de Atividade Física e Saúde [Internet]. 2016;21(2):110-22. doi: https://doi.org/10.12820/rbafs.v.21n2p110-122
22. Creswell JW, Creswell JD. Research design: Qualitative, quantitative, and mixed methods approaches. 5th ed. Los Angeles: SAGE Publications; 2018. 304 p.
23. Instituto Brasileiro de Geografia e Estatística (IBGE) [Internet]. Rio de Janeiro: Serviços e Informações do Brasil; c2024. Cities and States; 2024 [cited 2023 Dec 12]; [about 3 screens]. Available from: https://www.ibge.gov.br/en/cities-and-states.html?view=municipio
24. Sanchez C, Grzenda A, Varias A, Widge AS, Carpenter LL, McDonald WM, et al. Social media recruitment for mental health research: A systematic review. Compr Psychiatry [Internet]. 2020;103:152197. doi: https://doi.org/10.1016/j.comppsych.2020.152197
25. Matsudo S, Araújo T, Matsudo V, Andrade D, Andrade E, Oliveira LC, et al. Questionário Internacional de Atividade Física (IPAQ): Estudo de validade e reprodutibilidade no Brasil. Rev Bras Ativ Fis Saúde [Internet]. 2001;6(2):5-18. Available from: https://rbafs.org.br/rbafs/article/view/931
26. Lovibond PF, Lovibond SH. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther [Internet]. 1995;33(3):335-43. doi: https://doi.org/10.1016/0005-7967(94)00075-U
27. Vignola RCB, Tucci AM. Adaptation and validation of the depression, anxiety and stress scale (DASS) to Brazilian Portuguese. J Affect Disord [Internet]. 2014;155:104-9. doi: https://doi.org/10.1016/j.jad.2013.10.031
28. Santos AO. Capoeira Arte-Luta Brasileira. Cascavel: Assoeste; 2001. 173 p.
29. Levin K. Aesthetics of hyperactivity: A study of the role of expressive movement in ADHD and capoeira. Am. J. Dance Ther. [Internet]. 2016;38:41-62. doi: https://doi.org/10.1007/s10465-016-9211-7
30. Campos JADB, Martins BG, Campos LA, Marôco J, Saadiq RA, Ruano R. Early psychological impact of the COVID-19 pandemic in Brazil: A national survey. J Clin Med [Internet]. 2020;9(9):1-14. doi: https://doi.org/10.3390/jcm9092976
31. Danielsen KK, Øydna MH, Strömmer S, Haugjord K. “It’s more than just exercise”: Tailored exercise at a community-based activity center as a liminal space along the road to mental health recovery and citizenship. Int J Environ Res Public Health [Internet]. 2021;18(19):1-18. doi: https://doi.org/10.3390/ijerph181910516
32. Huang TT, Liu CB, Tsai YH, Chin YF, Wong CH. Physical fitness exercise versus cognitive behavior therapy on reducing the depressive symptoms among community-dwelling elderly adults: A randomized controlled trial. Int J Nurs Stud [Internet]. 2015;52(10):1542-52. doi: https://doi.org/10.1016/j.ijnurstu.2015.05.013
33. Fattore GL, Amorim LD, Santos LM, Santos DN, Barreto ML. Personal-level and group-level discrimination and mental health: The role of skin color. J Racial Ethn Health Disparities [Internet]. 2018;5(5):1033-41. doi: https://doi.org/10.1007/s40615-017-0451-0
34. Suárez-Iglesias D, Miller KJ, Seijo-Martínez M, Ayán C. Benefits of pilates in parkinson’s disease: A systematic review and meta-analysis. Medicina [Internet]. 2019;55(8):1-14. doi: https://doi.org/10.3390/medicina55080476
35. Pereira MJ, Mendes R, Mendes RS, Martins F, Gomes R, Gama J, et al. Benefits of pilates in the elderly population: A systematic review and meta-analysis. Eur J Investig Health Psychol Educ [Internet]. 2022;12(3):236-68. doi: https://doi.org/10.3390/ejihpe12030018
36. Aladro-Gonzalvo AR, Machado-Díaz M, Moncada-Jiménez J, Hernández-Elizondo J, Araya-Vargas G. The effect of pilates exercises on body composition: A systematic review. J Bodyw Mov Ther [Internet]. 2012;16(1):109-14. doi: https://doi.org/10.1016/j.jbmt.2011.06.001
37. Khazaei M, Marszałek J, Aminzadeh R, Dehghani E, Azizi B. Benefits of pilates exercises on functional fitness and quality of life in older men: A quasi-experimental study. Balt J Health Phys Act [Internet]. 2024;16(1):3. doi: https://doi.org/10.29359/BJHPA.16.1.03
38. Jackson M, Kang M, Furness J, Kemp-Smith K. Aquatic exercise and mental health: A scoping review. Complement Ther Med [Internet]. 2022;66:102820. doi: https://doi.org/10.1016/j.ctim.2022.102820
39. Neiva HP, Faíl LB, Izquierdo M, Marques MC, Marinho DA. The effect of 12 weeks of water-aerobics on health status and physical fitness: An ecological approach. PLoS One [Internet]. 2018;13(5):e0198319. doi: https://doi.org/10.1371/journal.pone.0198319
40. Del Bianco M, Lovecchio N, Pirazzi A, Gatti A, Pellino VC, Cucco L, et al. Self-reported physical activity level, emotions, feelings and self-perception of older active women: Is the water-based exercise a better enhancer of psychophysical condition? Sport Sci Health [Internet]. 2023;19:1311-7. doi: https://doi.org/10.1007/s11332-023-01094-4
41. Andersen MH, Ottesen L, Thing LF. The social and psychological health outcomes of team sport participation in adults: An integrative review of research. Scand J Public Health [Internet]. 2018;47(8):832-50. doi: https://doi.org/10.1177/1403494818791405
42. Zimmer C, McDonough MH, Hewson J, Toohey AM, Din C, Crocker PRE, et al. Social support among older adults in group physical activity programs. J. Appl. Sport Psychol. [Internet]. 2023;35(4):658-79. doi: https://doi.org/10.1080/10413200.2022.2055223
43. Oh S, Lim JM, Kim Y, Kim M, Song W, Yoon B. Comparison of the effects of water- and land-based exercises on the physical function and quality of life in community-dwelling elderly people with history of falling: A single-blind, randomized controlled trial. Arch Gerontol Geriatr [Internet]. 2015;60(2):288-93. doi: https://doi.org/10.1016/j.archger.2014.11.001
44. Moreira SR, Teixeira-Araujo AA, Santos AO, Simoes HG. Ten weeks of capoeira progressive training improved cardiovascular parameters in male practitioners. J Sports Med Phys Fitness [Internet]. 2017;57(3):289-98. doi: https://doi.org/10.23736/S0022-4707.16.06030-8
45. Moreira SR, Oliveira AC, Armstrong A. Capoeira: Hypothesis on health rehabilitation and quality-of-life maintenance. Rev Assoc Med Bras [Internet]. 2022;68(11):1530-6. doi: https://doi.org/10.1590/1806-9282.20220360
46. Moreira SR, Carvalho FO, Moraes JFVN, Carvalho RGS, Araújo RC, Teixeira-Araújo AA, et al. Eight weeks of capoeira progressive training program increases flexibility of beginners. Sport Sci Health [Internet]. 2016;12:329-37. doi: https://doi.org/10.1007/s11332-016-0292-y
47. Lima Júnior JCC, Sampaio JMF, Silva KT, Goncalves RM, Sousa SM, Macedo LR, et al. O ensino da capoeira: aspectos motivacionais que estimulam adesão à modalidade no município de Crato, Estado do Ceará, Brasil. Res Soc Dev [Internet]. 2020;9(8):e700096390. doi: https://doi.org/10.33448/rsd-v9i8.6390