
Reference Equations for the Six-Minute Walk Test in Healthy Adults in Southwestern Colombia: a Cross-Sectional Study
Ecuaciones de referencia para la prueba de marcha de seis minutos en adultos sanos del suroccidente colombiano: un estudio transversal
Esther Cecilia Wilches-Luna, Hamilton Elías Rosero-Carvajal , Álvaro Javier Arias Balanta, Diana Marcela Quintero Medina, Mauricio Hernández-Carrillo, Jhonatan Betancourt Peña,
Abstract
Introduction. The six-minute walk test (6MWT) is a submaximal test to assess functional capacity for exercise. In Colombia, the distance of the 6MWT is compared with those predicted by reference equations from other countries. Besides, pedometric measurements have not been included in the test.
Objective. To establish reference values for the distance walked in the six-minute walk test (6MWT) and the equation according to sex in healthy people in the southwestern Colombia.
Methods. Observational, cross-sectional, and correlational study. There were 336 volunteers, 227 males, with no history of respiratory disease, cardiovascular disease, or comorbidities limiting gait. Subjects performed the 6MWT twice on the same day in the morning, 30 minutes apart. The pedometer was placed at the starting point; the laps, meters, and number of steps in each test were recorded, selecting the one with the best distance. Linear regression was performed to obtain the reference equations by sex, according to age, weight, height, and number of steps. The R2 was used as a measure of adjustment.
Results. The distance walked was greater in males compared to females (616.7 [p25-75: 566.1-657.0] vs 588.0 [p25-75: 544.5-640.0]; p = 0.008). Two equations were obtained by sex, for females with R2 = 0.54 and males with R2 = 0.42.
Conclusion. The distance walked in 6MWT in Colombian subjects was more remarkable in males than females. Height and steps were the most significant predictors of the 6MWT length in the regression equations for females and males, with R2 of 0.54 and 0.42, respectively.
Keywords
Exercise test; walking; exercise tolerance; reference values; rehabilitation; physical therapy; exercise; functional status; oxygen consumption.
Resumen
Introducción. La prueba de marcha de 6 minutos (PM6M) evalúa la capacidad del ejercicio funcional, y sus resultados son comparados con predichos calculados con ecuaciones de referencia de poblaciones de otros países. Además, la podometría no ha sido incluida en la prueba.
Objetivo. Desarrollar ecuaciones de referencia para la PM6M de una población sana (20 a 69 años) de Cali, Colombia.
Método. Estudio observacional transversal. Se incluyeron 336 voluntarios, 227 hombres, sin antecedentes de enfermedad respiratoria, cardiovascular o comorbilidades que limiten la marcha. Los sujetos realizaron la PM6M dos veces el mismo día, con intervalo de 30 minutos. El podómetro fue ubicado en el paciente en el punto de partida, y se registraron los metros y el número de pasos en cada prueba. Se realizó regresión lineal para obtener las ecuaciones de referencia por sexo, edad, peso, talla y número de pasos. Se empleó como medida de ajuste el R2.
Resultados. La distancia recorrida fue mayor en hombres en comparación con mujeres (616.7 [p25-75: 566.1-657.0] vs 588.0 [p25-75: 544.5-640.0]; p = 0.008). Se obtuvieron dos ecuaciones, según el sexo, mujeres con R2 = 0.54 y para hombres un R2 = 0.42.
Conclusión. La distancia recorrida en la PM6M en sujetos colombianos fue mayor en hombres. La talla y los pasos fueron las variables predictivas más significativas de la distancia en la PM6M en las ecuaciones de regresión para mujeres y hombres.
Palabras clave
Prueba de paso; prueba de esfuerzo; caminata; tolerancia al ejercicio; valores de referencia; rehabilitación; ejercicio físico; fisioterapia; consumo de oxígeno; estado funcional.
Introduction
The 6MWT is a sub-maximal test that assesses the systems involved in exercise and reflects the patient's behavior in activities of daily living. The 6MWT is recommended to evaluate the response to pharmacological and non-pharmacological therapeutic interventions, assess functional status, and predict survival/mortality in several diseases [1,2].
In some countries, studies were conducted on healthy individuals to determine the average values of the distance walked in 6MWT in the USA [3], Belgium [4], Portugal [5], and in the Chinese population [6], among others. In Latin America, some studies are well known, such as those carried out in Chile [7], Brazil [8], and Brazil, Santiago de Chile, Colombia, Pamplona, Santa Cruz de Tenerife Zaragoza, Montevideo, Boston Tampa, and Caracas by Casanova et al. [9].
In Colombia, although the 6WMT is routinely used in cardiac and pulmonary rehabilitation programs, reference equations designed for populations in other countries are used, with different anthropometric and ethnic characteristics that do not represent our population. Some authors suggest that variables such as sex, age, weight, and height are the main determinants of establishing predicted values of distance walked [3,4,10,11]. Therefore, it is necessary to carry out studies that show equations considering the anthropometric characteristics of our population to perform objective measurements in rehabilitation programs.
The 6MWT is a safe, inexpensive tool, and the equipment needed for its performance is few and easily acquired. In turn, some authors have used pedometers to assess the level of physical activity and its relationship with functional capacity [12]. Considering that pedometers are easily accessible technological devices, including them during the 6MW would facilitate the recording of the number of steps, providing additional information on the participant's performance and the changes generated by rehabilitation interventions. These arguments allow us to justify the inclusion of pedometrics as a new variable in the proposed baseline equations for the 6MWT.
Currently, no known studies determine reference equations to predict the distance walked in the 6MWT with a representative sample of a healthy Colombian population. Therefore, this study aimed to establish the reference values of the distance walked in the 6MWT in a healthy population of southwestern Colombia and determine a reference equation according to sex, age, anthropometric measurements, and the number of steps covered. All of this to provide a tool that will allow health professionals in our region to have reliable parameters to perform objective evaluations and establish interventions tailored to the needs of the patients.
Method
An observational, cross-sectional, and correlational study was conducted in 2017 and 2018. The sample consisted of the population of the city of Santiago de Cali, to 1000masl.
Healthy subjects over 18 years of age, with the absence of musculoskeletal injuries, with no history of hospitalization during the six weeks before the study, with Charlson index 0, residents of the city of Cali older than six months, who were able to walk independently were included [13]. Subjects with chronic respiratory, cardiovascular, metabolic, neuromuscular, rheumatologic, or musculoskeletal diseases that influenced the ability to walk independently were excluded.
Sample size calculation
The correlation between the variables sex, weight, height, the number of steps, and the 6MWT was estimated using the following formula:
$$ n = \left( \frac{Z_{1 - \alpha/2} + Z_{1 - \beta}}{\frac{1}{2} \cdot \ln\left(\frac{1 + r}{1 - r}\right)} \right)^2 + 3 $$
Where (r) is the estimated population correlation. After a bibliographic search, no similar studies in Colombia provided such information. Therefore, estimates were taken from a study conducted with healthy subjects aged 20 to 80 in Chile [7]. The criterion used was the geographical proximity between Chile and Colombia and the assumption of a more significant anthropometric similarity between the subjects of these two countries compared with studies at the world level.
The study by Osses et al. made it possible to identify estimates of correlations differentiated by sex, and the lowest reported coefficients were chosen for the sample size [7]. The reliability (1-α) was 95% (α = 0.05), and the 1-β statistical power established for this study was 80% (β = 0.2). The following values associated with the normal distribution were considered for the bilateral case: Z_(1-α⁄2) =1.96 and Z_(1-β) = 0.84. The minimum size required to estimate these correlations was 426 participants. At the end of the study, a sample of 322 participants (225 men and 97 women) was obtained, reaching a final reliability for men of 90% and a statistical power of 80%. In the case of women, a reliability of 93.25% and a statistical power of 80% were obtained.
Ethical considerations
The study was approved by the Ethics Committee of the Universidad del Valle, Colombia (approval act 06-014) and by the Institutional Committee where the tests were performed, under the Helsinki declaration. On the day of the 6MWT, all participants signed the informed consent form, and a copy was provided. Each participant was assigned a code to preserve the confidentiality of the information.
Procedures
The media were used to recruit participants, and direct contact was established with community members who received information about the study. Communication was maintained by e-mail and telephone, informing participants of the days on which the tests would be carried out and the recommendations of ATS for the 6MWT [10].
Height and weight were obtained according to techniques standardized by the World Health Organization, with the participants in light clothing and without shoes. They were measured with a calibrated Health o Meter Professional® scale (0.1kg accuracy), 350lb/160kg capacity, and a measuring rod or stadiometer (0.5cm accuracy). Weight and height were used to calculate the body mass index (BMI).
Before and at the end of the 6MWT, heart rate, peripheral oxygen saturation (SpO2), respiratory rate, blood pressure, and the perception of dyspnea and fatigue (were monitored with the modified Borg scale), in a sitting position. Heart rate and SpO2 were monitored during the test via wireless telemetry (WEP-4208J®Nihon Kohden Corporation).
The test was performed in a flat corridor 30 meters long, with a cone at each end, and the participants were stimulated every minute with standardized phrases until completing 6 minutes. All participants performed two tests on the same day, in the morning, with a 30-minute break. The laps and meters walked in each test were recorded, and the one with the longest distance walked was selected for analysis [10].
The pedometer, Omron Hj-720itffp poket® brand, was placed according to some authors' recommendations: perpendicular to the floor, on the right hip, and once the participant was at the starting line [14]. The pedometer was removed at the end of each test, and the number of steps was recorded, being calibrated before use to ensure the reliability of the information.
All measurements were performed by two physiotherapists specializing in Cardiopulmonary Physiotherapy, with three years of experience in the performance of the test and with training in user instructions, verbal commands, use of forms, and taking of variables.
Statistical methods
A data quality verification process was carried out, with a weekly review of the information recorded in the forms. The report was then entered in Excel and verified by an external person. For the description of the data, the Kolmogorov-Smirnov test was initially applied to find out whether the data behaved according to a normal distribution. If the assumption of normality was not met, the variables were reported as medians as a measure of central tendency with their respective interquartile range as a measure of variability. The Mann-Whitney U test was used to compare variables by sex.
The study variables were evaluated to determine the degree of linear association with the 6MWT, which was measured using Pearson's correlation test. In addition, a multiple linear regression analysis was performed to evaluate the contribution of the independent variables to the estimation of the distance walked in the 6MWT, for which sex, age, weight, height, and the number of steps were considered as predictor variables. The adjusted R2 was taken into account to measure the model fit.
The assumptions of the regression model were duly validated using the Shapiro Wilk test to validate the normality of the residuals, the Levene test to evaluate the homogeneity of the variance of the residuals, and the Durbin Watson test to check the non-correlation of the residuals.
Data analysis was performed in Stata statistical software version 14. A p-value <0.05 was considered statistically significant throughout the study.
Results
Table 1 presents that, in the comparison by sex, age, and steps covered in the 6MWT were similar in males and females (p = 0.705 and p = 0.423 respectively), in contrast to height, weight, and BMI, which presented statistically significant differences (p = 0.000, p = 0.000, and p = 0.012 respectively). The distance walked in the 6MWT showed statistically significant differences (p = 0.009).
Table 1. Comparison of characteristics by sex.
| Variable | P Value* | ||
|---|---|---|---|
| n = 225 | n = 97 | ||
| Age (years) | 44.0 (30.0 - 55.0) | 42 (28.0- 54.0) | 0.71 |
| Height (cm) | 172.0 (166.0 - 177.0) | 159.0 (156.0 - 163.0) | <0.001 |
| Weight (kg) | 79.0 (70.0 - 87.5) | 64.0 (58.0 - 73.5) | <0.001 |
| BMI (Kg/m2) | 26.9 (24.3- 29.9) | 25.9 (23.1-28.3) | 0.01 |
| Steps performed | 758.0 (714.0-791.0) | 764.0 (725.0-796.0) | 0.42 |
| Distance walked in the 6MWT (m) | 616.7 (566.1 - 657) | 588.0 (544.5 - 640) | 0.009 |
Notes. Data presented in Median (p25-75). *Statistical test: Mann-Whitney U test. P-value < 0.05. BMI: Body Mass Index; 6MWT: six-minute walk test.
Figure 1 shows that, for the median distance walked by a group of age and sex, with increasing age, the distance decreased to a greater extent for women. Starting with a median of 610.0m for the age range 20-29 years, and at ages 60-69 years, the distance decreased to 546m; while in men, the change was 646.5m in the age range 20-29 years and 592.5m for men 60-69 years. However, these differences were not statistically significant for men (p = 0.329) and women (p = 0.181).
Figure 1. Median distance walked by a group of age and sex.

Figure 2 presents the evaluation of the correlation between the independent variables and the distance in the 6MWT, showing that age demonstrated a weak correlation of 0.27, and height showed a higher correlation of (r = 0.35). Concerning weight, no linear relationship was identified (r = 0.06). As for the number of steps, the variable showed the highest correlation with the distance walked (r = 0.54).
Figure 2. Correlation between predictor variables with the response variable.
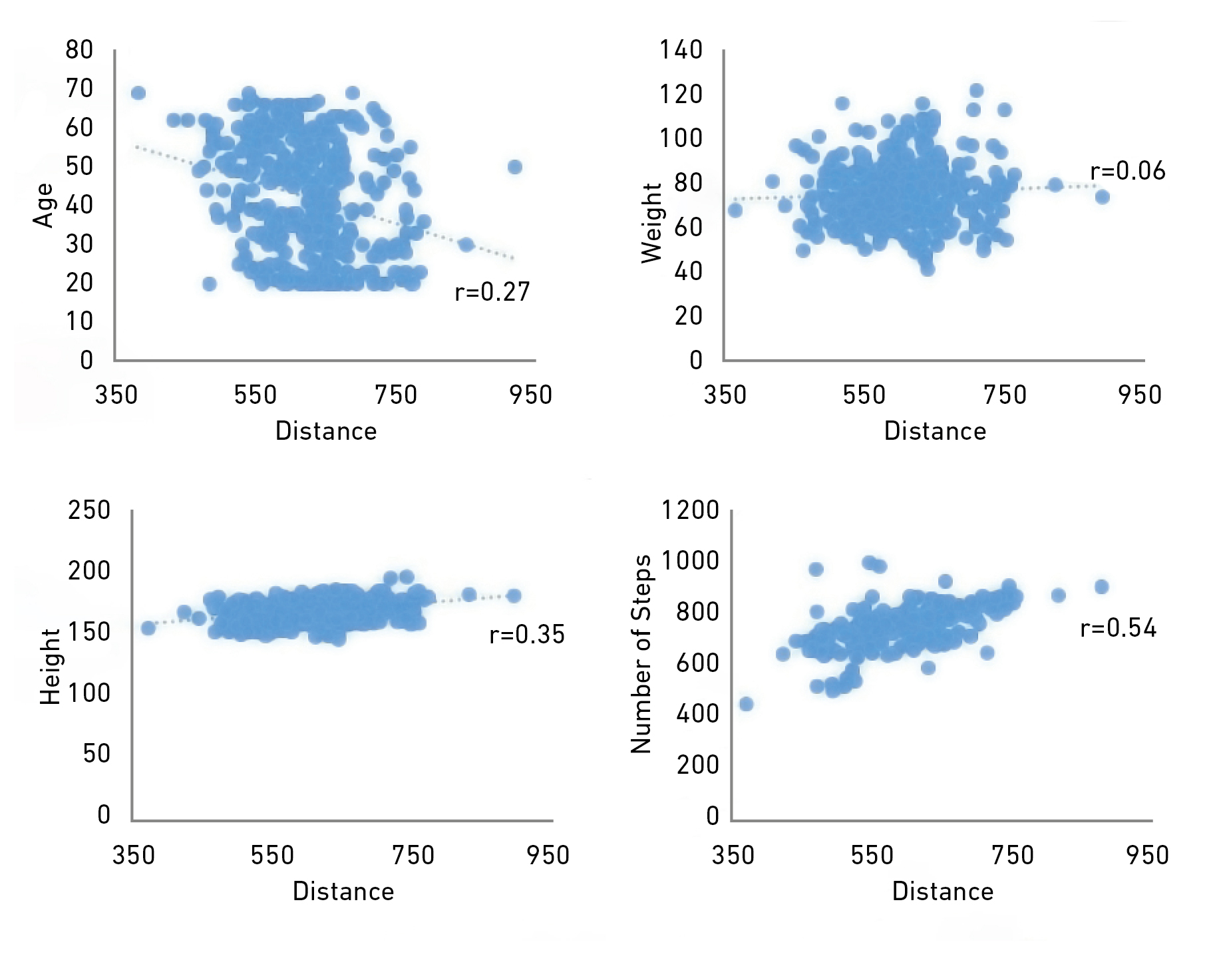
Note. Correlation between predictor variables (age, weight, height, and number of steps) with the response variable (distance in the 6MWT).
Reference equations
Table 2 shows that equations were established for estimating the distance walked in the 6MWT for men and women between 20 and 69 years of age. In the multiple linear regression models, age, weight, height, and the number of steps for women and men were included, obtaining an adjusted R2 of 0.54 and 0.42, respectively. All the variables included were significant in females; the variables of weight, height, and steps were statistically significant in males (p = 0.036, p = 0.000, and p = 0.000, respectively).
Table 2. Multiple regression models for the 6MWT according to sex. Age range between 20 and 69 years.
| Variables | Female (n = 97) | |
|---|---|---|
| Coefficient | P Value | |
| Age | -0.88 | 0.02 |
| Weight | -2.94 | <0.001 |
| Height | 3.84 | <0.001 |
| Steps | 0.35 | <0.001 |
| Constant | -48.61 | 0.74 |
| R2 Adjusted | 0.54 | <0.001 |
| Multiple Model* 6MWT | (-0.88 x ageYears) - (2.94 x WeightKg) + (3.84 x Height cm) + (0.35 x StepsNum) - 48.61cm | |
| Variables | Male (n = 225) | |
| Coefficient | P Value | |
| Age | -0.05 | 0.86 |
| Weight | -0.75 | 0.04 |
| Height | 3.98 | <0.001 |
| Steps | 0.65 | <0.001 |
| Constant | -493.5 | <0.001 |
| R2 Adjusted | 0.42 | <0.001 |
| Multiple Model* 6MWT | (-0.05x AgeYears) - (-0.75x WeightKg) + (3.98x Heightcm) + (0.65x StepsNum) - 493.5cm | |
Note. 6MWT: six-minute walk test.
Discussion
The study aimed to establish reference values for the distance walked in the 6MWT and the equation according to sex in healthy people in the southwestern part of Colombia. The results showed that it was possible to design two equations, one for women and one for men, with R2 of 0.54 and 0.42, respectively, using age, weight, height, and the number of steps as predictive variables.
Clinicians and researchers can use this information in the study's region. Nevertheless, currently, equations developed in other countries are used. Therefore, it is recommended that reference values of the population where the test is performed be used for interpretation [10,15,16]. Hence, the researchers of this study consider that the equations obtained could be the most appropriate for evaluating functional capacity in this population.
Two tests were performed with standardized minute-by-minute orientations, and the best distance walked was taken for the analysis [10,17]. In the methodology described in the study by Enright and Sherrill [3], they performed a single attempt, and participants received no stimulus during the test. In the present study, two tests were performed with the stimulus to walk as fast as possible, as in the studies by Troosters et al. in Belgium and Osses et al
Concerning using the pedometer during the test, according to the review by Miragall et al. [19], all pedometers are accurate at moderate speeds, regardless of the location. In this study, it was placed perpendicular to the ground, on the right hip, and no difficulty was presented in terms of falls or displacements during the performance of the two tests. The authors of this study agree with Miragall et al. [19] in that the characteristics of the pedometers vary considerably according to model and location, so it is always necessary to use the same device and consider explicit and complete information on the model used, and the spot indicated. Literature related to the 6MWT in different pathologies and contexts is growing; however, there is scarce literature describing the use of the pedometer during the test to compare the results and favor the reliability of the information.
In this study with the southwestern Colombian population, the distance walked in the 6MWT was 616.7m. for men and 588.0m. for women, results similar to those published by Walteros et al., who found 658.9m. in men and 592.7m in women; and
In the southwest of Colombia, in cardiac and pulmonary rehabilitation programs, prediction equations are used to calculate the distance walked in the 6MWT, designed with populations from other countries [3,4], which could be causing over or underestimation of the predicted distance, influencing the therapeutic goals established in the rehabilitation programs. In this regard, Mendoza-Núñez et al. and Bernal-Orozco et al. suggest that the development, validation, and application of equations that include anthropometric data should be performed in the local population with a similar social context to minimize estimation errors [26,27]. The previous information supports this study's results that considered the subjects' sociodemographic and anthropometric characteristics and required specific equations.
The results of the distance walked in the 6MWT can vary in populations with similar anthropometric characteristics. Casanova et al. compared healthy men and women from seven countries. The results showed that for each geographic area, there are differences between the variables, finding a significant decrease in the distance in the older population. In terms of sex, they found that men walked 30 meters more than women [9]. Results similar to those identified in the present study, in which a more significant difference of 28.7m was observed in men compared to the distance walked by women. The authors of this study consider that these results could be explained by the fact that men are taller than women, finding a difference of 13cm in height, which proportionally increases the length of the stride. In addition to the above, men present more significant development of muscle mass and strength [5,28,29].
In the Chilean population, the results reported were significantly higher in men than in women, 644±84 vs. 576±87m, respectively, and in Brazil, the mean distance walked in the 6MWT for the second test was 583±83m (range: 417-828m); results very similar to those of the present study 616.7m (566.1-657.0) and 588.0m (544.5-640.0) for men and women, respectively, considering that the population of these countries have anthropometric characteristics similar to the city where the present study was conducted.
In this investigation, the regression equation showed that height and weight were significant predictors for the distance walked in the 6MWT for both sexes (p<0.001). Data that coincide with the studies of Trossters et al. and Rikli et al. with Caucasian subjects found greater height and distance walked in the 6MWT compared with the results obtained in Asian and Saudi populations [4,22-24,30]. The differences between countries can also be influenced by various factors, such as the altitude above sea level. This study shows a good tolerance of the population associated with the test without significant alteration of vital signs, ethnicity, population selection criteria, and the methodology for performing the test [24,31].
The differences in the results of the 6MWT can also be explained by a critical parameter related to the step length for walking since those who have a longer walking length must turn more frequently and spend more time moving. This study presents a significant advance in the analysis of the results linking the steps performed to complement this analysis.
The studies reviewed also describe the design of prediction equations using anthropometric variables such as weight and height; however, the number of steps was not included [3,4,7,15]. To date, no known studies in southwestern Colombia have included the use of pedometry in the performance of the 6MWT. The authors consider that pedometry can be proposed as a practical and economical method to complement the evaluation of the reference values obtained through the 6MWT and to facilitate the follow-up of physical activity [32].
Regarding the number of steps performed in the 6MWT, healthy subjects demonstrated a relationship with the distance walked that is not even modified with different instructions given by the evaluator, which implies that this variable can be considered to perform the 6MWT routinely and used as a reference value in this population [33,34].
The authors consider as a strength of the study that the same evaluator performed all measurements in the same period of the day. The evaluator also followed the same protocol to reduce the occurrence of discrepancies and biases during data collection, the probability of error in the proposed equations, and the quality control performed in the data collection and analysis processes. Integrating podometry into the proposed equations introduces an innovative approach to evaluating functional capacity using the 6MWT.
Limitations are related to greater participation of men than women, implying that one of the groups could have greater representativeness; however, the results reported represent our population. Further multi-center validation studies are recommended to facilitate comparison between different people and to support the use of the proposed equations in the clinical setting
Conclusions
Men had a greater distance walked in the 6MWT compared to women. Height and steps were the most significant predictors of the 6MWT length in the regression equations for females and males, with R2 of 0.54 and 0.42, respectively. In the regression equations for men and women, height and steps were the most significant predictors for 6MW walking distance, with R2 of 0.54 and 0.42, respectively.
This study is a reference framework in southwestern Colombia, a pioneer in including podometry and establishing equations for predicting the distance covered in the 6MWT test, considering anthropometric variables specific to the population.
These equations could be a tool for the evaluation and monitoring of rehabilitation interventions. However, additional studies are required to validate these results and identify the applicability of the equations in clinical contexts.
References
1. Solway S, Brooks D, Lacasse Y, Thomas S. A qualitative systematic overview of the measurement properties of functional walk tests used in the cardiorespiratory domain. Chest [Internet]. 2001;119(1):256-70. doi: https://doi.org/10.1378/chest.119.1.256
2. VanWagner LB, Harinstein ME, Runo JR, Darling C, Serper M, Hall S, et al. Multidisciplinary approach to cardiac and pulmonary vascular disease risk assessment in liver transplantation: An evaluation of the evidence and consensus recommendations. Am J Transplant [Internet]. 2018;18(1):30-42. doi: https://doi.org/10.1111/AJT.14531
3. Enright P, Sherrill D. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med [Internet]. 1998;158(5 Pt 1):1384-7. doi: https://doi.org/10.1164/AJRCCM.158.5.9710086
4. Troosters T, Gosselink R, Decramer M. Six minute walking distance in healthy elderly subjects. Eur Respir J [Internet]. 1999;14(2):270-4. doi: https://doi.org/10.1034/J.1399-3003.1999.14B06.X
5. Oliveira M, Marçôa R, Moutinho J, Oliveira P, Ladeira I, Lima R, et al. Reference equations for the 6-minute walk distance in healthy Portuguese subjects 18-70 years old. Pulmonology [Internet]. 2019;25(2):83-9. doi: https://doi.org/10.1016/J.PULMOE.2018.04.003
6. Zou H, Zhang J, Chen X, Wang Y, Lin W, Lin J, et al. Reference Equations for the Six-Minute Walk Distance in the Healthy Chinese Han Population, Aged 18-30 Years. BMC Pulm Med [Internet]. 2017;17(1):119. doi: https://doi.org/10.1186/S12890-017-0461-Z
7. Osses R, Yáñez J, Barría P, Palacios S, Dreyse J, Díaz O, et al. Prueba de caminata en seis minutos en sujetos chilenos sanos de 20 a 80 años. Rev Med Chile [Internet]. 2010;138(9):1124-30. doi: https://doi.org/10.4067/S0034-98872010000900006
8. Sperandio EF, Arantes RL, Matheus AC, Silva RP, Lauria VT, Romiti M, et al. Intensity and physiological responses to the 6-minute walk test in middle-aged and older adults: a comparison with cardiopulmonary exercise testing. Braz J Med Biol Res [Internet]. 2015;48(4):349-53. doi: https://doi.org/10.1590/1414-431X20144235
9. Casanova C, Celli BR, Barria P, Casas A, Cote C, de Torres JP, et al. The 6-min walk distance in healthy subjects: Reference standards from seven countries. Eur Respir J [Internet]. 2011;37(1):150-6. doi: https://doi.org/10.1183/09031936.00194909
10. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am J Respir Crit Care Med [Internet]. 2002;166(1):111-7. doi: https://doi.org/10.1164/ajrccm.166.1.at1102
11. de Souza SAF, Faintuch J, Fabris SM, Nampo FK, Luz C, Fabio TL, et al. Six-minute walk test: functional capacity of severely obese before and after bariatric surgery. Surg Obes Relat Dis [Internet]. 2009;5(5):540-3. doi: https://doi.org/10.1016/J.SOARD.2009.05.003
12. Wan E, Kantorowski A, Homsy D, Teylan M, Kadri R, Richardson C, et al. Promoting physical activity in COPD: Insights from a randomized trial of a web-based intervention and pedometer use. Respir Med [Internet]. 2017;130:102-10. doi: https://doi.org/10.1016/J.RMED.2017.07.057
13. Iwama AM, Andrade GN, Shima P, Tanni SE, Godoy I, Dourado VZ. The six-minute walk test and body weight-walk distance product in healthy Brazilian subjects. Braz J Med Biol Res [Internet]. 2009;42(11):1080-5. doi: https://doi.org/10.1590/S0100-879X2009005000032
14. Holbrook EA, Barreira TV, Kang M. Validity and Reliability of Omron Pedometers for Prescribed and Self-Paced Walking. Med Sci Sport Exerc [Internet]. 2009;41(3):670-4. doi: https://doi.org/10.1249/MSS.0b013e3181886095
15. Dourado VZ. Equações de referência para o teste de caminhada de seis minutos em indivíduos saudáveis. Arq Bras Cardiol [Internet]. 2011;96(6):e128-38. doi: https://doi.org/10.1590/S0066-782X2011005000024
16. Rosero Carvajal HE, Cuero-Campáz DF, Arias-Balanta AJ, Wilches Luna EC. Distancia recorrida en la prueba de marcha de los 6 minutos en una población caleña sana de entre 20 y 65 años. Estudio piloto. Rehabilitación [Internet]. 2017;51(3):143-8. doi: https://doi.org/10.1016/J.RH.2016.12.003
17. Holland AE, Spruit MA, Troosters T, Puhan MA, Pepin V, Saey D, et al. An official European respiratory society/American thoracic society technical standard: Field walking tests in chronic respiratory disease. Eur Respir J [Internet]. 2014;44(6):1428-46. DOI: https://doi.org/10.1183/09031936.00150314
18. Gibbons W, Fruchter N, Sloan S, Levy R. Reference values for a multiple repetition 6-minute walk test in healthy adults older than 20 years. J Cardiopulm Rehabil [Internet]. 2001;21(2):87-93. doi: https://doi.org/10.1097/00008483-200103000-00005
19. Miragall M, Domínguez A, Cebolla A, Baños RM. El uso de podómetros para incrementar la actividad física en población adulta: una revisión. Clínica y Salud [Internet]. 2015;26(2):81-9. doi: https://doi.org/10.1016/J.CLYSA.2015.06.002
20. Walteros Manrique RE. Distancia recorrida de la prueba de caminata de seis minutos en población adulta sana en una comunidad universitaria de la ciudad de Bogotá [master’s thesis]. Bogotá (CU): Universidad Nacional de Colombia; 2018. p. 1-62.
21. Viola Muñoz LC. Valores normales de referencia de la prueba de marcha de seis minutos (P6M) en adultos sanos mayores de 18 años en Bogotá, Colombia [master’s thesis]. Bogotá (CU): Universidad de La Sabana; 2015. p. 1-23. Available from: http://hdl.handle.net/10818/17826
22. Poh H, Eastwood PR, Cecins NM, Ho K, Jenkins SC. Six-minute walk distance in healthy Singaporean adults cannot be predicted using reference equations derived from Caucasian populations. Respirology [Internet]. 2006;11(2):211-6. doi: https://doi.org/10.1111/J.1440-1843.2006.00820.X
23. Teramoto S, Ohga E, Ishii T, Yamaguchi Y, Yamamoto H, Mastsuse T. Reference value of six-minute walking distance in healthy middle-aged and older subjects. Eur Respir J [Internet]. 2000;15(6):1132-3. doi: https://doi.org/10.1034/J.1399-3003.2000.01525.X
24. Mosharraf-Hossain AKM, Chakrabortty R. Reference values of 6 minutes walk test (6 MWT) in Bangladeshi healthy subjects aged 25-55 years. Bangladesh Med Res Counc Bull [Internet]. 2014;40(2):70-3. doi: https://doi.org/10.3329/BMRCB.V40I2.25224
25. Alameri H, Al-Majed S, Al-Howaikan A. Six-min walk test in a healthy adult Arab population. Respir Med [Internet]. 2009;103(7):1041-6. doi: https://doi.org/10.1016/J.RMED.2009.01.012
26. Mendoza-Nún̈ez VM, Sánchez-Rodríguez MA, Cervantes-Sandoval A, Correa-Muñoz E, Vargas-Guadarrama LA. Equations for predicting height for elderly Mexican Americans are not applicable for elderly Mexicans. Am J Hum Biol [Internet]. 2002;14(3):351-5. doi: https://doi.org/10.1002/AJHB.10029
27. Bernal-Orozco MF, Vizmanos B, Hunot C, Flores-Castro M, Leal-Mora D, Cells A, et al. Equation to estimate body weight in elderly Mexican women using anthropometric measurements. Nutr Hosp [Internet]. 2010;25(4):648-55. Available from: https://scielo.isciii.es/scielo.php?pid=S0212-16112010000400018&script=sci_abstract&tlng=pt
28. Kim AL, Kwon JC, Park I, Kim JN, Kim JM, Jeong BN, et al. Reference equations for the six-minute walk distance in healthy korean adults, aged 22-59 years. Tuberc Respir Dis (Seoul) [Internet]. 2014;76(6):269-75. doi: https://doi.org/10.4046/TRD.2014.76.6.269
29. Palaniappan Ramanathan R, Chandrasekaran B. Reference equations for 6-min walk test in healthy Indian subjects (25-80 years). Lung India [Internet]. 2014;31(1):35-8. doi: https://doi.org/10.4103/0970-2113.125892
30. Rikli RE, Jones CJ. Functional Fitness Normative Scores for Community-Residing Older Adults, Ages 60-94. J Aging Phys Act [Internet]. 1999;7(2):162-81. doi: https://doi.org/10.1123/JAPA.7.2.162
31. Gibson OR, Richardson AJ, Hayes M, Duncan B, Maxwell NS. Prediction of physiological responses and performance at altitude using the 6-minute walk test in normoxia and hypoxia. Wilderness Environ Med [Internet]. 2015;26(2):205-10. doi: https://doi.org/10.1016/J.WEM.2014.11.004
32. Ehrler F, Weber C, Lovis C. Influence of Pedometer Position on Pedometer Accuracy at Various Walking Speeds: A Comparative Study. J Med Internet Res [Internet]. 2016;18(10):e5916. doi: https://doi.org/10.2196/JMIR.5916
33. Southard V, Gallagher R. The 6MWT. Will different methods of instruction and measurement affect performance of healthy aging and older adults? J Geriatr Phys Ther [Internet]. 2013;36(2):68-73. doi: https://doi.org/10.1519/JPT.0B013E318264B5E8
34. Muñoz-Cofré R, Sol Md, Lizana PA, Gómez-Bruton A, Fuentes Andaur MJ, Fierro ES, et al. Comparison of distance covered, physiological cost, and perceived exertion in four six-minute walk test protocols. Front. Physiol [Internet]. 2024;15:1395855. doi: https://doi.org/10.3389/fphys.2024.1395855