Creation of various Pediatric Vocal Self-Assessment Questionnaires Worldwide: a Scoping Review
Creación de diversos cuestionarios de autoevaluación vocal pediátrica a nivel mundial: una revisión de alcance
Soledad Correa , Renata Azevedo, Millaray Alfaro Bugueño, Paula Urbina, Alexandra Varas González, Valentina Vásquez Castillo
Abstract
Introduction. Childhood dysphonia can affect emotionally, socially and/or academically the infant's life, so it is essential to obtain a complete evaluation at vocal level, considering voice self-assessment.
Objective. To know and describe the characteristics of pediatric vocal self-assessment instruments created worldwide.
Method. A review of the scope was conducted in accordance with the methodologically established search criteria. The data analysis was performed after the search in several scientific database platforms. Twelve articles were incorporated into the final review and, based on the results obtained, 17 vocal self-evaluation questionnaires were described, indicating their evaluation objectives, structural conformation, target population, country of creation, methodological construction and psychometric characteristics.
Results. 17 original vocal self-assessment questionnaires were found, published in Italian, English, Portuguese, and Spanish. The studies considered several vocal pathologies and variable age ranges, including population from 0 to 21 years of age, The sample used was variable, with 3 publications with an experimental group of less than 100 subjects. 4 investigations presented adaptations of questionnaires originally created for adult voice and 2 investigations presented abbreviations of original questionnaires for pediatric voice. Considering the description of psychometric measures, 1 questionnaire presented sensitivity and specificity, 2 questionnaires presented validity and reliability, 4 questionnaires presented only reliability, 6 questionnaires presented specificity, sensitivity, and efficiency, and 4 questionnaires described reliability, validity, specificity, and sensitivity.
Conclusion. 17 original pediatric vocal self-assessment questionnaires were identified and described.
Keywords
Surveys and questionnaires; self-assessment; voice; dysphonia; quality of life; minors; child; psychometrics.
Resumen
Introducción. La disfonía infantil puede afectar emocional, social y/o académicamente la vida del infante, por lo que es fundamental obtener una evaluación completa a nivel vocal, considerando la autoevaluación de voz.
Objetivo. Conocer y describir las características de los instrumentos de autoevaluación vocal pediátrica creados a nivel mundial.
Método. Se llevó a cabo una revisión de alcance conforme a los criterios de búsqueda establecidos metodológicamente. El análisis de los datos fue llevado a cabo posterior a la búsqueda en diversas plataformas de bases de datos científicas. Se incorporaron a la revisión final 12 artículos y, a partir de los resultados obtenidos, se describieron 17 cuestionarios de autoevaluación vocal, indicando sus objetivos de evaluación, conformación estructural, población objetivo, el país de creación, construcción metodológica y sus características psicométricas.
Resultados. Se hallaron 17 cuestionarios de autovaloración vocal originales, publicados en los idiomas italiano, inglés, portugués y español. Los estudios consideraron diversas patologías vocales y rangos etarios variables, incluyendo a población de entre 0 a 21 años de edad. La muestra utilizada fue variable, incluyendo 3 publicaciones con grupo experimental menor a 100 sujetos. 4 investigaciones presentaron adaptaciones de cuestionarios creados originalmente para voz adulta y 2 investigaciones presentaron abreviaciones de cuestionarios originales para voz pediátrica. Considerando la descripción de las medidas psicométricas, 1 cuestionario presentó sensibilidad y especificidad, 2 cuestionarios presentaron validez y confiabilidad, 4 cuestionarios presentaron solo confiabilidad, 6 cuestionarios presentaron especificidad, sensibilidad y eficiencia, sumado a 4 cuestionarios que describieron confiabilidad, validez, especificidad y sensibilidad.
Conclusión. Se identificaron y describieron 17 cuestionarios originales de autoevaluación vocal pediátrica.
Palabras clave
Encuestas y cuestionarios; autoevaluación; voz; disfonía; calidad de vida; menores; niño; psicometría.
Introduction
During infancy, abusive vocal behavior can generate different phonatory deviations, transitory or chronic, that influence the daily life of children of different ages [1]. Although dysphonia at the pediatric level is difficult to detect because it often goes unnoticed due to the changes experienced during growth [2], some voice alteration at an early age could have a negative impact on the child's life, being effective a timely detection [3]. The presence of dysphonia causes concern in the child's family circle since emotional, social, and academic aspects may be affected, which could influence their quality of life [4].
Childhood dysphonia is caused by inadequate vocal behavior due to phonotrauma and initially manifests itself as a laryngeal malfunction, which if sustained over time could lead to a benign organic-functional lesion, with nodules being the most common lesion in the school stage, with an incidence of 17%-30% [5].
The speech-language pathologist is in charge of establishing the presence and degree of severity of a voice alteration through a comprehensive evaluation; a section of this corresponds to the vocal self-assessment questionnaires, through which information is obtained about the perception that people have about their voice and how it impacts on their quality of life [6]. With this information, it is possible to plan a more specific intervention for each patient, taking into consideration the results obtained in the questionnaires [7].
Since the voice is the main means of communication, it is advisable to use self-assessment tools in the clinic, considering they provide information on how this alteration affects the child's daily life. For this reason, the need arises to know the pediatric vocal self-assessment questionnaires that have been created worldwide and if they comply with the psychometric measures established for their construction. To respond to the above-mentioned, a scope review will be carried out to describe the characteristics of the questionnaires found.
Method
The design of this research is a scoping review that allows for a broad or detailed description of a topic, exploring all studies that are related to the research question [8]. This type of review aims to identify the scope and nature of the existing literature on a topic in the available research [9]. Thus, the scoping review allows for answering a broader question compared to a systematic review and performs a thorough search in terms of the methodology of the available scientific evidence, which differentiates it from a narrative review. This research seeks to know all the pediatric vocal self-assessment questionnaires that have been created and published to date, along with describing their psychometric properties.
This review did not include chronological restriction, because we sought to analyze all published articles that indicate the creation of a pediatric vocal self-assessment questionnaire. The papers that were selected included the target population between 0 and 21 years of age, people of both sexes, and with presence of vocal pathology. Studies originally published in English, Italian, Portuguese, and Spanish were selected, as well as publications translated into English from their original language. Psychometric research related to the creation of pediatric vocal self-assessment questionnaires was analyzed, being of a descriptive and exploratory qualitative nature and quantitative in its descriptive scope. Single case studies, literature reviews, linguistic and cultural adaptations, and psychometric studies not related to the topic of pediatric voice were excluded.
The databases used to collect the information were Scopus, SciELO, WOS, and PubMed with the search terms MESH related to evaluation questionnaires, voice, and pediatric population. The search terms, Boolean operators, and cross-referencing are shown in Table 1.
Table 1. Search terms and Boolean operators.
| Natural language terms | MESH terms and Boolean operators |
|---|---|
| Self-assessment questionnaires | "surveys and questionnaires" OR "patient reported outcome measures" OR "patient outcome assessment" OR "self-assessment". |
| AND | |
| Voice | "voice disorders" OR "voice" OR "dysphonia" OR "phonation" OR "voice quality". |
| AND | |
| Pediatric population | "pediatrics" OR "pediatric" OR "minors" OR "child" OR "adolescent" OR "children". |
Note. eaning of AND: AND; meaning of OR : OR.
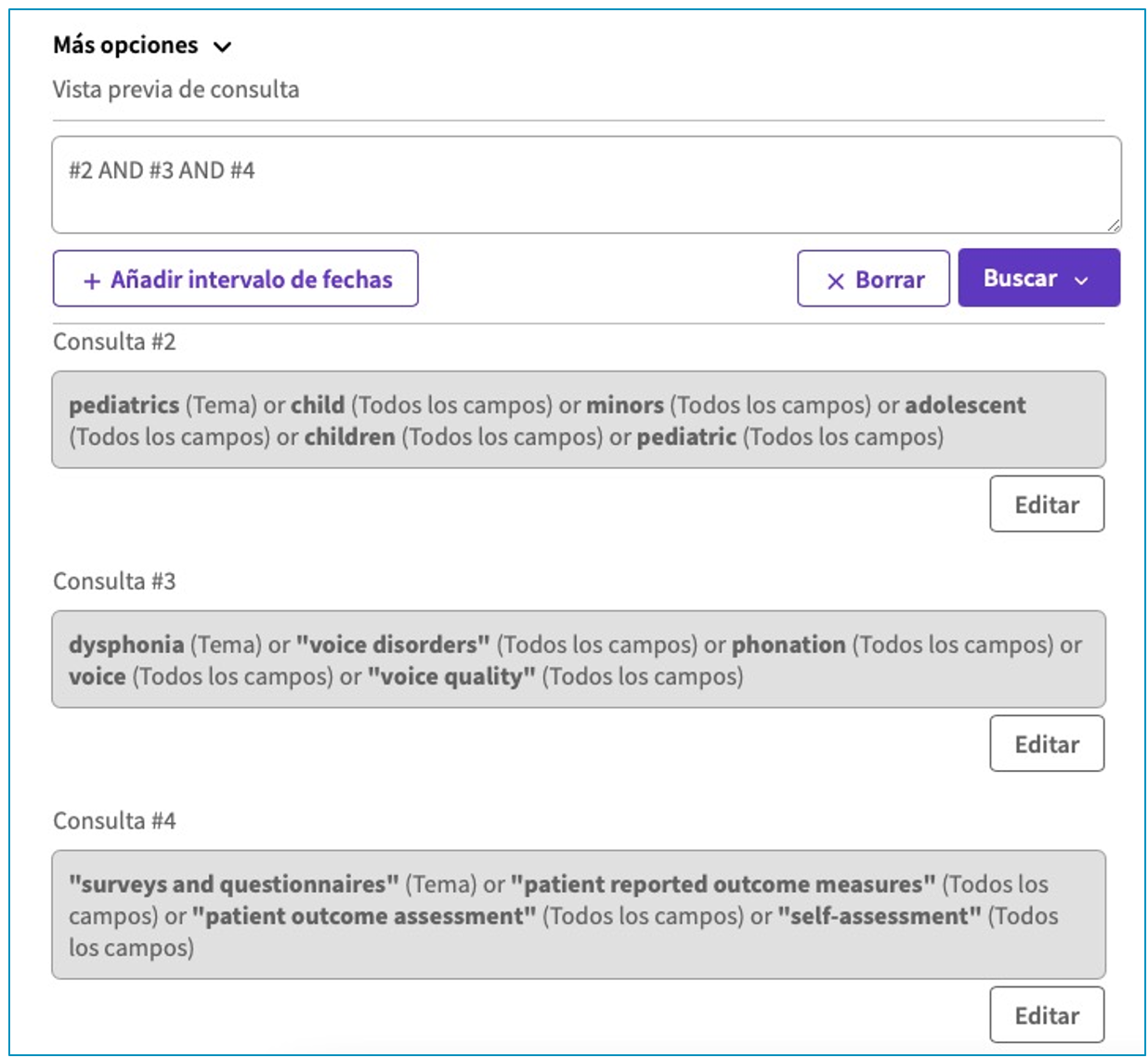
The filters applied were as follows for all databases:
1 Expression 1: (pediatrics) or (child) or (minors) or (adolescent) or (children) or (pediatric).
2 Expression 2: (dysphonia) or ("voice disorders") or (phonation) or (voice) or ("voice quality).
3 Expression 3: ("surveys and questionnaires) or ("patient reported outcome measures") or ("patient outcome assessment") or (self-assessment).
4 #1 and #2 and #3.
The support of the search for each database is shown in Appendix: Figures A, B, C, and D.
The Rayyan® platform was used to organize the search results. The search for studies resulted in a total of 508 articles, with 230 articles indexed in PubMed, 216 in Scopus, 61 in WOS, and 1 in SciELO. 61 duplicate articles were recorded, leaving 447 documents for review of titles and abstracts, and 429 were subsequently excluded. The full text of the remaining 18 articles was read, of which 6 were excluded; 4 of them because they did not include the pediatric population, 1 because it was not exclusively for the pediatric population and 1 because its objective was not the creation of a questionnaire, but to establish the psychometric measures of a previously created questionnaire. Finally, 12 articles were included in the present review. The publications found range from 2002 to 2023. The selection process described above is shown in the PRISMA flowchart [10] (Figure 1), where it is evident that the search and selection followed the inclusion and exclusion criteria mentioned above.
Figure 1. PRISMA Flowchart [10]
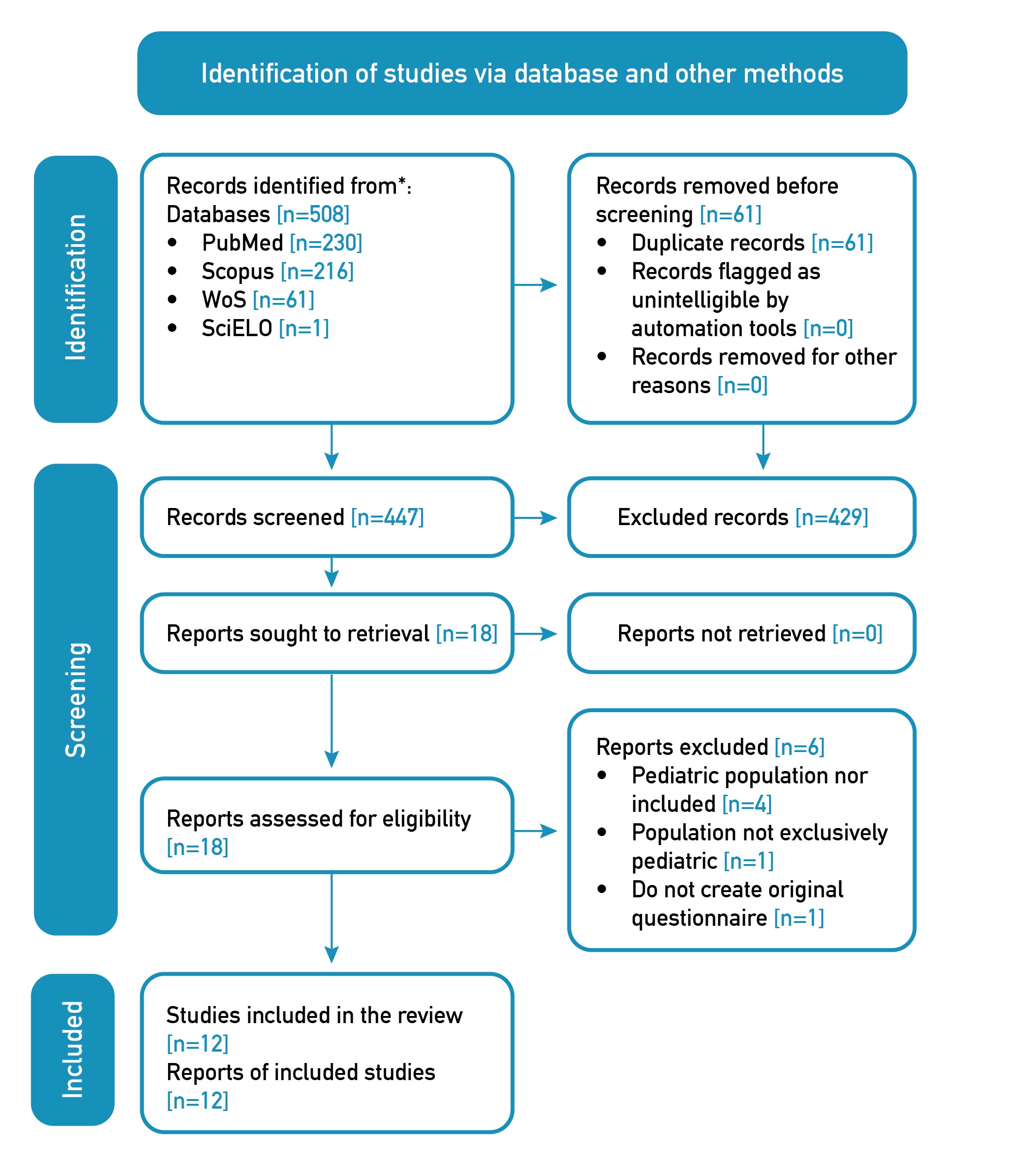
Nota. Note. Adapted from The PRISMA 2020 statement: an updated guideline for reporting systematic reviews [10].
Results
The articles found and selected for the scoping review were as follows: Validation of a Pediatric Voice Quality-of-Life Instrument: The Pediatric Voice Outcome Surve [11]; Validation of the Pediatric Voice-Related Quality-of-Life Survey [12]; Pediatric Voice Handicap Index (pVHI): A new tool for evaluating pediatric dysphonia [13]; Glottal Function Index: A Predictor of Glottal Disorders in Children [14]; Validation and Standardization of the Pediatric Voice Symptom Questionnaire: A Double-Form Questionnaire for Dysphonic Children and Their Parents [15]; Development and Validation of the Children's Voice Handicap Index-10 (CVHI-10) [16]; Development and Validation of the Children's Voice Handicap Index-10 for Parents [17]; Parent and Child Responses to the Pediatric Voice-Related Quality-of-Life Questionnaire [18]; Development and validation of a short version of the Spanish pediatric voice handicap index (P-VHI-10) [19]; Pediatric Vocal Symptoms Questionnaire (PVSQ): Four new versions for parental evaluation and self-evaluation [20]; Development, Validation, and Reliability of the Teacher-Reported Pediatric Voice Handicap Index [21]; and Development and Validation of the Children's Voice Questionnaire (CVQ) [22].
The characteristics of each research study and questionnaire created are detailed below. This information is grouped in Table 2.
Table 2. Characteristics of each investigation and questionnaire created.
| Title | Author(s) | Year | Country | Target | Participants | Questionnaire | Measurement Objective | Number Of Items | Domains | Response Options | Population | Age Range | Respondent | Cutoff Score | Psychometric Characteristics |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Validation of a Pediatric Voice Quality-of-Life Instrument the Pediatric Voice Outcome Survey [11] | Hartnik | 2002 | United States | To validate a parent instrument to study voice-related quality of life in the pediatric population. | 108 caregivers or parents of children with tracheostomy or decannulation | Pediatric Voice Outcome Survey (P-VOS) | Quality of Life in the pediatric population | 4 | --- | Vocal quality Likert scale (item 1) (excellent to my child has no voice) Likert scale of vocal limitation (item 2) (very limited to not limited at all) Likert scale of quantity (items 3 and 4) (not at all to extremely) | Children and adolescents who had a tracheotomy or were surgically decannulated | 2 to 18 years | Parents or caregivers or guardians | 49.8+-27.1 (0 - 100) | Reliability of the instrument for the range of 2 to 18 years: 0.83 (Cronbach's alpha) Reliability of the instrument for the range of 2 to 5 years: 0.86 (Cronbach's alpha) Reliability of the instrument for the range of 6 to 10 years: 0.85 (Cronbach's alpha) Reliability of the instrument for the range of 11 to 18 years: 0.69 (Cronbach's alpha) Construct validity: p=0.004 |
| Validation of the Pediatric Voice-Related Quality-of-Life Survey [12] | Boseley et al. | 2006 | United States | Validate the Pediatric Voice-Related Quality-of-Life survey, which was designed to assess voice changes over time in the pediatric population. | 120 parents of children with dysphonia | Pediatric Voice-Related Quality-of-Life Survey (P-VRQOL) | Voice-related quality of life in the pediatric population. | 10 | Socio-emotional and physical-functional | Likert scale of quality (not a problem to the problem is as bad as it could be). | Children and adolescents with various otorhinolaryngological pathologies. | 2 to 18 years | Parents | 91.1 | Instrument Reliability: 0.96 (Cronbach's alpha) Test-Retest Reliability: 0.80 (Cronbach's alpha) Convergent Validity: 0.70 (p<0.001) Discriminant Validity: p<0.001 |
| Pediatric Voice Handicap Index (pVHI): A new tool for evaluating pediatric dysphonia [13] | Zur et al. | 2007 | United States | Adapt the Voice Handicap Index to the pediatric population and validate it. | 78 parents of children and adolescents with and without dysphonia | Pediatric Voice Handicap Index (P-VHI) | Effects of dysphonia in the pediatric population. | 23 | Physical, Functional and Emotional |
Numerical scale from 1 to 7 to assess talkativeness Likert frequency scale (never to always) Visual analog scale to evaluate the degree of vocal severity (normal to severe). |
Children and adolescents seeking laryngotracheal reconstruction and subsequent treatment. Children with dysphonia not related to airway problems. |
3 to 21 years | Parents or caregivers or guardians |
Physical Scale Control Group: 0.20 Functional Scale Control Group: 1.47 Emotional Scale Control Group: 1.47 Total Control Group: 1.84 Physical Scale Experimental Group: 15.48 Functional Scale Experimental Group: 13.94 Emotional Scale Experimental Group: 12.15 Total Experimental Group: 41.58 EAV Experimental Group: 52.91 |
Test-retest reliability Physical Component: r = 0.77 (p<0.001) (Pearson's correlation) Test-retest reliability Functional Component: r = 0.95 (p<0.001) (Pearson's correlation) Test-retest reliability Emotional Component: r = 0.79 (p<0.001) (Pearson's correlation)001 (Pearson's correlation) Test-retest reliability Emotional Component: r = 0.79 (p<0.001) (Pearson's correlation) Test-retest reliability Visual Analog Scale: r = 0.71 (p=0.002) (Pearson's correlation) Reliability of the total instrument with the Functional and Emotional component: 0.86 (Pearson correlation). Reliability of the total instrument with the Physical component: 0.59 (Pearson correlation). Reliability between degree of severity indicated in the Visual Analog Scale and total score: r=0.66 (Pearson correlation). |
| Glottal Function Index: A Predictor of Glottal Disorders in Children [14] | Cohen et al. | 2007 | Israel | To evaluate the efficacy of the Glotal Function Index in the detection of vocal cord disorders in children. | 100 father/mother and son/daughter pairs | Glottal Function Index adapted to pediatric population | Detect alterations in vocal folds | 4 | --- | Numerical scale from 0 to 5 points of severity (not a problem to severe problem). | Children and adolescents with organic and behavioral dysphonia | 2 to 16 years old | Parents |
Control group: 2.5 +- 3.88 Experimental Group: 7.2+- 5.6 |
Specificity: 72%. Sensitivity: 70%. |
| Validation and Standardization of the Pediatric Voice Symptom Questionnaire: A Double-Form Questionnaire for Dysphonic Children and Their Parents [15] | Ingrid et al. | 2012 | Belgium | Validate the Pediatric Voice Symptom Questionnaire that is presented with a parallel form for children and their parents. | 375 participants
•42 infants •333 father/mother and son/daughter pairs |
Pediatric Voice Symptom Questionnaire (PVSQ) |
Vocal symptoms in the pediatric population | 31 | --- |
Likert frequency scale (never to always) Visual support of circles of different sizes from small to very large for the response of the child population. |
Children and adolescents with dysphonia | 6 to 18 years | Parents/caregivers and infants. | --- |
Internal consistency child-response version: 0.879 (Cronbach's alpha). Internal consistency parent-response version: 0.893 (Cronbach's alpha). Consistency Test-Retest version answered by children: 0.876 (Cronbach's alpha). Consistency Test-Retest version answered by parents: 0.757 (Cronbach's alpha). Construct validity for children: r=0.884 (p<0.000). Construct validity for parents: r=0.811 (p<0.000). Sensitivity and Specificity for both questionnaires:
• Non-dysphonic < Dysphonic = p<0.001 Total score correlation between children and parents:
• Non-dysphonic: 0.055 (p=0.187) (Spearman's correlation) • Dysphonics: 0.478 (p<0.001) (Spearman correlation) |
| Development and Validation of the Children's Voice Handicap Index-10 (CVHI-10) [16] | Ricci-Maccarini et al. | 2013 | Italy | Develop and validate the self-administered Children's Voice Handicap Index-10 for children and evaluate its internal consistency and reliability in normal and dysphonic children's voices. | 136 infants |
Children's Voice Handicap Index-10 (CVHI-10) |
Vocal disadvantage in pediatric population | 10 | --- | Likert frequency scale (never to always) | Children with dysphonia. | 8 to 14 years old | Infants | Experimental group: 10.4 +-3.2 |
Internal consistency of the instrument: 0.85 (Cronbach's alpha). Test-retest reliability: r=0.84 (p<0.001) (Pearson correlation). Construct validity: • Correlation between CVHI-10 and PVHI: r=0.74 (p<0.001) (Wilcoxon test). • Pre- and post therapy: p>0.001 (Wilcoxon test) Sensitivity: • Degree of dysphonia: r=0.62 (Spearman correlation). >• Hoarseness: r=0.38 (Spearman's correlation) • Soplocity: r=0.34 (Spearman's correlation) Specificity: p>0.001 (Mann-Whitney U test) |
| Development and Validation of the Children's Voice Handicap Index-10 for Parents [17] | Ricci-Maccarini et al. | 2016 | Italy | Develop and validate an assessment tool parallel to the CVHI-10 for parents to assess the level of vocal impairment in their child's voice. | 55 father/mother and son/daughter pairs | Children's Voice Handicap Index-10 for Parents (CVHI-10-P) | Vocal disadvantage in pediatric population | 10 | --- | Likert frequency scale (never to always) | Children with dysphonia | 8 to 14 years old | Parents | --- |
Internal consistency: 0.78 (Cronbach's alpha) Correlation between CVHI-10 and CVHI-10-P: r=0.37 |
| Parent and Child Responses to the Pediatric Voice-Related Quality-of-Life Questionnaire [18] | Cohen et al. | 2015 | Scotland | Conduct a pilot study of an adaptation of the Pediatric Voice-Related Quality-of-Life Questionnaire. | 24 father/mother/son/daughter pairs | Pediatric Voice-Related Quality-of-Life Questionnaire adapted for children | Voice-related quality of life in the pediatric population. | 10 | Socio-emotional and physical-functional |
Likert scale of quality (not a problem to the problem is as bad as it could be). Range of pictograms graded from a crying face to a very happy face |
Children and adolescents with dysphonia | 3 to 15 years | Infants and adolescents | --- |
Test-Retest Reliability: • Socioemotional component: r=0.85 • Physical-functional component:r=0.77 • Total: r=0.87 Correlation of children and parents by scores • Socioemotional component: r=0.72 • Physical-functional component:r=0.67 • Total: r=0.76 |
| Development and validation of a short version of the Spanish pediatric voice handicap index (P-VHI-10) [19] | Sanz et al. | 2016 | Spain | Develop and validate a short Spanish version of the P-VHI (P-VHI-10) and evaluate whether it is comparable to the Italian C-VHI-10. | 27 parents of children and adolescents with dysphonia | Short version of the Spanish pediatric voice handicap index (P-VHI-10) | Vocal disadvantage in pediatric population | 10 | Physical and functional | Likert frequency scale (never to always) | Children and adolescents with dysphonia | 6 to 15 years | Parents | Experimental group: 18.7+-7.45 |
Comparison between PVHI total score and PVHI-10: 0.602 (p<0.36) (T Student). Internal consistency:0.75 (Cronbach's alpha) |
| Pediatric Vocal Symptoms Questionnaire (PVSQ): Four new versions for parental evaluation and self-evaluation [20] | Lima et al. | 2020 | Brazil | To develop reduced versions of the Pediatric Vocal Symptoms Questionnaire (PVSQ) protocol for the two forms of application of the instrument: self-assessment (SA) and parental evaluation (PE). |
367 children and adolescents with and without dysphonia 349 parents or caregivers of children and adolescents with and without dysphonia |
Common Core of the Pediatric Vocal Symptoms Questionnaire Self-evaluation | Vocal symptoms in the pediatric population | 26 | Vocal performance, vocal effort, vocal fatigue, pain symptoms, limitation in vocal activities, phonatory symptoms and socio-emotional symptoms. | Likert scale of frequency (never to always) and visual support of circles of different sizes from small to very large for the response of the child population. | Children and adolescents with dysphonia | 6 to 18 years | Infants | 4.45 |
Specificity:0.898 Sensitivity: 0.405 Efficiency: 0.652 |
| Common Core of the Pediatric Vocal Symptoms Questionnaire Parental Evaluation | 20 | Vocal performance, vocal effort, vocal fatigue, pain symptoms, limitation in vocal activities. | Likert frequency scale (never to always) | Children and adolescents with dysphonia | 6 to 18 years | Parents | 1.45 |
Specificity:0.815 Sensitivity: 0.495 Efficiency: 0.655 |
|||||||
| Common Core of the Pediatric Vocal Symptoms Questionnaire Self-evaluation Reduced version | 10 | Vocal performance, vocal effort, vocal fatigue, pain symptoms, limitation in vocal activities, phonatory symptoms and socio-emotional symptoms. | Likert scale of frequency (never to always) and visual support of circles of different sizes from small to very large for the response of the child population. | Children and adolescents with dysphonia | 6 to 18 years | Infants | 2.75 |
Specificity:0.841 Sensitivity: 0.548 Efficiency: 0.695 |
|||||||
| Common Core of the Pediatric Vocal Symptoms Questionnaire Parental Evaluation Reduced version | 10 | Vocal performance, vocal effort, vocal fatigue, pain symptoms, limitation in vocal activities. | Likert frequency scale (never to always) | Children with dysphonia. | 6 to 18 years | Parents | 1.75 |
Specificity:0.885 Sensitivity: 0.386 Efficiency: 0.636 |
|||||||
| Pediatric Vocal Symptoms Questionnaire Self-evaluation reduced version | 10 | --- | Likert scale of frequency (never to always) and visual support of circles of different sizes from small to very large for the response of the child population. | Children and adolescents with dysphonia | 6 to 18 years | Infants | 2.75 |
Specificity:0.860 Sensitivity: 0.448 Efficiency: 0.654 |
|||||||
| Pediatric Vocal Symptoms Questionnaire Parental evaluation reduce version | 15 | --- | Likert frequency scale (never to always) | Children and adolescents with dysphonia | 6 to 18 years | Parents | 1.91 |
Specificity:0.904 Sensitivity: 0.357 Efficiency: 0.631 |
|||||||
| Development, Validation, and Reliability of the Teacher-Reported Pediatric Voice Handicap Index [21] | Yağcıoğlu et al. | 2022 | Turkey | To develop a new teacher-reported pediatric voice outcome measure and investigate its psychometric properties. | 306 father/mother/son/daughter/teacher/child pairs | Teacher-Reported Pediatric Voice Handicap Index(TRPVHI) | Vocal disadvantage in the pediatric population. | 27 | Functional, physical and emotional | Likert frequency scale (never to always) | Children and adolescents with dysphonia | 4 to 11 years | Teachers | --- |
Content validity Instrument: 0.9
Content validity of the Functional scale: 0.89 Content validity of the Physical scale: 0.89 Content validity of the Emotional scale: 0.923 (factor analysis). Construct validity of the Functional scale: 0.96 (factor analysis) Construct validity of the Physical scale: 0.94 (factor analysis). Construct validity of Emotional scale: 0.96 (factor analysis). Criterion validity of the instrument: 0.65 (Pearson correlation). Functional scale criterion validity: 0.47 (Pearson's correlation) Criterion validity of the Physical scale: 0.68 (Pearson correlation). Emotional scale criterion validity: 0.51 (Pearson correlation). Internal Consistency Instrument: 0.98 (Cronbach's alpha) Internal consistency of functional scale: 0.94 (Cronbach's alpha). Internal consistency of Physical scale: 0.96 (Cronbach's alpha). Internal consistency of Emotional scale: 0.94 (Cronbach's alpha). Test-retest reliability Instrument: 0.98 (P<0.001) (Pearson's correlation) Test-retest reliability of Functional scale: 0.91 (P<0.001) (Pearson correlation). Physical scale test-retest reliability: 0.98 (P<0.001) (Pearson correlation). Test-retest reliability of Emotional scale: 0.96 (P<0.001) (Pearson correlation). Sensitivity and specificity: p<0.001 (Mann Whitney U test). |
| Development and Validation of the Children's Voice Questionnaire (CVQ) [22] | Amir et al. | 2023 | Israel | Develop and validate the Children's Voice Questionnaire, a self-administered instrument for children. | 342 infants and adolescents |
Children's Voice Questionnaire (CVQ) |
Perception of dysphonia and on voice-related quality of life in the pediatric population. | 18 | --- | Likert frequency scale (never to always) | Children and adolescents with dysphonia | 7 to 18 years old | Infants and adolescents |
Control Group: 4.2 +-5.58 Experimental group: 14.66 +-14.06 |
Internal consistency:0.94 (Cronbach's alpha) Test-retest reliability: r=0.79 (P<0.001) Construct validity:(0.59 < r < 0.66, P < 0.01). Sensitivity and specificity: (t[78.25] = 6.22, P < 0.001) ( t test). |
Validation of a Pediatric Voice Quality-of-Life Instrument: The Pediatric Voice Outcome Survey [11] is a study that aimed to validate an instrument for parents to study voice-related quality of life in the pediatric population. This study was conducted in the United States on 108 caregivers or parents of children and adolescents aged 2 to 18 years with tracheostomy or decannulation. The research develops the Pediatric Voice Outcome Survey (P-VOS). It presents as psychometric characteristics good reliability in general by age range of 0.83 (2 to 18 years), 0.86 (2 to 5 years), 0.85 (6 to 10 years), 0.69 (11 to 18 years), which is on the borderline of being questionable. Regarding construct validity, it presents p = 0.004, which indicates that it is statistically significant. The Pediatric Voice Outcome Survey (P-VOS) is established for the population of children and adolescents who had tracheotomy or were surgically decannulated between 2 and 18 years of age; it has 4 items and no domains. It seeks to measure the quality of life in the pediatric population and its answers are measured by means of a Likert scale of vocal quality (item 1; excellent to my child has no voice); Likert scale of vocal limitation (item 2; very limited to not limited at all); Likert scale of quantity (items 3 and 4; not at all to extremely) and has a cut-off score for the dysphonic population of 49.8+-27.1 points. This questionnaire is answered by parents or caregivers.
Validation of the Pediatric Voice-Related Quality-of-Life Survey [12] aims to validate the Pediatric Voice-Related Quality-of-Life (PVRQOL) survey, which was designed to evaluate voice changes over time in the pediatric population. The study was conducted in the United States with 120 parents of children and adolescents aged 2 to 18 years with a variety of otolaryngologic diagnoses, including disorders affecting the voice. The research develops the Pediatric Voice-Related Quality-of-Life Survey (P-VRQOL), which presents a good instrument reliability of 0.96 and good test-retest reliability of 0.80. As for construct validity, a convergence of 0.70 (<0.001) and discriminant p<0.001 were obtained, making it a valid instrument. The Pediatric Voice-Related Quality-of-Life survey (P-VRQOL) is established for a population of children and adolescents with dysphonia, aged 2 to 18 years, to measure voice-related quality of life; it has 10 items and 2 domains: socioemotional and physical-functional. Its response options are through a Likert scale of quality (it is not a problem to the problem is as bad as it could be) and has a cut-off score of 91.1 points for the pediatric population. This questionnaire is answered by parents or caregivers.
Pediatric Voice Handicap Index (pVHI): A new tool for evaluating pediatric dysphonia [13] aimed to adapt the VHI to the pediatric population and validate it. This study was conducted in the United States with 78 parents of children and adolescents aged 3 to 21 years with and without dysphonia. The research developed the Pediatric Voice Handicap Index (P-VHI) questionnaire, which presents a positive test-retest reliability of the physical domains of r = 0.77, functional of r = 0.95, and emotional of r = 0.79, in addition to the visual analog scale of r = 0.71. The reliability of the total instrument, considering the functional and emotional domains, is 0.86, with a positive correlation and high association between the two variables. Finally, the reliability between the degree of severity indicated in the visual analog scale and the total score is r = 0.66, also showing a positive correlation. The Pediatric Voice Handicap Index (P-VHI) questionnaire is established for the population of children and adolescents seeking laryngotracheal reconstruction and subsequent treatment or children with dysphonia not related to airway problems, both groups between 3 and 21 years of age. It seeks to measure the effects of dysphonia in the pediatric population. It presents 23 items, with three domains: physical, functional, and emotional; its response options are a numerical scale from 1 to 7 to evaluate loquacity, a Likert scale of frequency (never to always), and a visual analog scale to evaluate the degree of vocal severity (normal to severe). Regarding their scores, the control group presented 0.20 points for the physical domain, 1.47 points for the functional, 1.47 points for the emotional, and a total score of 1.84 points. For the experimental group, the cut-off score for the physical domain is 15.48 points, for the functional is 13.94 points, for the emotional is 12.15 points, and the total cut-off score is 41.58 points. The cut-off score for the visual analog scale for the experimental group is 52.91 points. This questionnaire is answered by parents or caregivers.
Glottal Function Index (GFI): A Predictor of Glottal Disorders in Children [14] aimed to evaluate the efficacy of the Glottal Function Index [23] adapted for the pediatric population in the detection of vocal cord disorders in children. This study was conducted in Israel on 100 children aged 2 to 16 years undergoing flexible fiberoptic laryngoscopy, where a GFI survey was given to the parents of each participant in the study. Regarding its psychometric measures, the sensitivity of the GFI was 70% and the specificity 72%; thus, the questionnaire has an adequate detection of a person with pathology and a person without pathology. The Glottal Function Index questionnaire adapted to the pediatric population is established for children and adolescents with organic and behavioral dysphonia age between 2 to 16 years and seeks to detect alterations in the vocal folds; it presents 4 items and does not have domains. It is answered through a numerical scale from 0 to 5 points of severity (not a problem to a severe problem) and has a cut-off score of 2.5 points (+- 3.88) for the control group and 7.2 points (+- 5.6) for the experimental group. This questionnaire is answered by parents or caregivers.
The study called Validation and Standardization of the Pediatric Voice Symptom Questionnaire: A Double-Form Questionnaire for Dysphonic Children and their Parents aimed to validate the Pediatric Voice Symptom Questionnaire (PVSQ) [15], which is presented with a parallel form for children and parents. This research was conducted in Belgium with 375 participants, which were 42 infants aged 5 to 13 years and 333 father/mother and son/daughter pairs. It presents adequate internal consistency both in the version answered by children, which is 0.87, and in the one answered by parents, which is 0.89. In the test-retest, a value of 0.87 was obtained in the children's version and 0.75 in the parents' version, which means both are reliable. It presents adequate construct validity both for children, which is r = 0.88 (p<0.000), and parents, which is r = 0.81 (p<0.000). The sensitivity and specificity for both questionnaires is between children without dysphonia lower than children with dysphonia = p<0.001, indicating that there is a significant difference between the groups, i.e., the capacity to identify true positives and true negatives is significant. The research developed the Pediatric Voice Symptom Questionnaire (PVSQ) [16], which is intended for a population of children and adolescents with dysphonia aged 6 to 18 years and seeks to describe vocal symptoms. This questionnaire has 31 items and no domains and is answered through a Likert scale of frequency (never to always) and visual support of circles of different sizes from small to very large for the response of the child population. The questionnaire is answered by both parents and children and adolescents with dysphonia.
Development and Validation of the Children's Voice Handicap Index-10 (CVHI-10) [16] aimed to develop and validate the self-administered Children's Voice Handicap Index-10 for children and to evaluate its internal consistency and reliability in children with healthy and pathological voices. This study was conducted in Italy with a sample of 136 infants in the age range of 8 to 14 years. The Children's Voice Handicap Index-10 (CVHI-10) questionnaire is established for children with dysphonia aged 8 to 14 years and seeks to measure vocal handicap in the pediatric population; it presents 10 items, without specific domains, with response option through the Likert frequency scale (never to always) and has a cut-off score for the experimental group of 10.4 (+-3.2) points. The overall perceptual assessment scores of the 51 children after vocal therapy improved considerably, showing a statistically significant reduction of the total score and for each item in CVHI-10 after vocal therapy. The questionnaire is answered by the children themselves.
Development and Validation of the Children's Voice Handicap Index-10 for Parents [17] is a study that aimed to develop and validate an assessment tool parallel to the CVHI-10 for parents to assess the level of vocal handicap in their children's voice. This study was conducted in Italy with a sample of 55 parent-child pairs ranging in age from 7 to 12 years. The research developed the Children's Voice Handicap Index-10 for Parents (CVHI-10-P) questionnaire, which has a good internal consistency of 0.78; the correlation between CVHI-10 and CVHI-10-P is low, with a value of r = 0.37. The overall results yielded a lower CVHI-10-P total score than the CVHI-10 in most cases. Single-item mean scores were always lower in CVHI-10-P compared to CVHI-10, except for the one CVHI-10-P item directly involving parental experience (item 10). The data obtained with one tool are not directly related to the other, suggesting that these two tools assess the child's voice disability from different perspectives. The Children's Voice Handicap Index-10 for Parents questionnaire [17] is established for parents of children with dysphonia aged 8 to 14 years. It seeks to measure vocal handicap in the pediatric population; it presents 10 items, without specific domains, with response option through frequency Likert scale (never to always). No cut-off scores are reported in the publication, although a statistically significant reduction of the total score, and for each item in CVHI-10-P after vocal therapy, is evidenced. This questionnaire is answered by parents or caregivers.
Parent and Child Responses to the Pediatric Voice-Related Quality-of-Life Questionnaire [18] aimed to conduct a pilot study of an adaptation of the Pediatric Voice-Related Quality-of-Life Questionnaire (PVRQoL) to be answered by the same pediatric population. This study was conducted in Scotland with 24 father/mother/son/daughter pairs, ranging in age from 3 to 15 years. About its psychometric measures, according to test-retest reliability, the socioemotional domain is r = 0.85, the physical-functional domain is r = 0.77, and the total is r = 0.87, indicating high reliability. Regarding the correlation between the questionnaires for children and parents, the socioemotional domain is r = 0.72, the physical-functional domain is r = 0.67, and the total result is r = 0.76, indicating a good reliability of the instrument. The Pediatric Voice-Related Quality-of-Life Questionnaire adapted for children is designed for children and adolescents with dysphonia aged 3 to 15 years to assess voice-related quality of life. It presents 10 items with two domains, one socioemotional and one physical-functional, and is answered through a Likert scale of quality (not a problem to the problem is as bad as it could be) plus a range of pictograms graduated between them, from a crying face to a very happy face to facilitate children's response. No cut scores are reported in the publication. The questionnaire is answered by the children themselves.
The study called Development and validation of a short version of the Spanish pediatric voice handicap index (P-VHI-10) [19] aimed to develop and validate a short Spanish version of the P-VHI (P-VHI-10) and to evaluate whether it is comparable with the Italian C-VHI-10. This study was conducted in Spain with 27 parents of children and adolescents aged 6 to 15 years with a diagnosis of dysphonia. The internal consistency is 0.75, which means that it presents adequate reliability. The comparison between the total score of the PVHI and PVHI-10 is 0.60 (p<0.36), which indicates that the observed difference is not statistically significant. The questionnaire Short version of the Spanish pediatric voice handicap index (P-VHI-10) [19] seeks to evaluate vocal handicap in the pediatric population aged 6 to 15 years with a diagnosis of dysphonia. It presents 10 items with two domains, physical and functional, and is answered through a Likert frequency scale (never to always). The experimental group presents an overall cut-off score of 18.7 (+-7.45) points. This questionnaire is answered by parents or caregivers.
Pediatric Vocal Symptoms Questionnaire (PVSQ): Four new versions for parental evaluation and self-evaluation is a study [20] that aimed to develop reduced versions of the Pediatric Vocal Symptoms Questionnaire (PVSQ) [15] for the two forms of application of the instrument: self-evaluation and parental evaluation. This study was conducted in Brazil with 367 children and adolescents aged 6 to 18 years with and without dysphonia and with 349 parents or caregivers of children and adolescents with and without dysphonia. The research developed the following questionnaires: Common Core of the Pediatric Vocal Symptoms Questionnaire Self-evaluation, presenting an adequate specificity of 0.89 and a non-discriminant sensitivity of 0.40, thus obtaining a poor overall discriminant efficiency of 0.6; Common Core of the Pediatric Vocal Symptoms Questionnaire Parental Evaluation, with an adequate specificity of 0.81 and a non-discriminant sensitivity of 0.49, therefore obtaining a poor overall discriminant efficiency of 0.65; Common Core of the Pediatric Vocal Symptoms Questionnaire Self-evaluation Reduced version, presenting an adequate specificity of 0.84 and a non-discriminant sensitivity of 0.54, which obtains a poor overall discriminant efficiency of 0.69; Common Core of the Pediatric Vocal Symptoms Questionnaire Parental Evaluation Reduced version, with an adequate specificity of 0.88 and a non-discriminant sensitivity of 0.38, getting a poor overall discriminant efficiency of 0.63; Pediatric Vocal Symptoms Questionnaire Self-evaluation Self-evaluation Reduced version, presenting an adequate specificity of 0.86 and a non-discriminant sensitivity of 0.44, thus obtaining an overall poor discriminant efficiency of 0.65; Pediatric Vocal Symptoms Questionnaire Parental evaluation Reduced version, with a high specificity of 0.90 and a non-discriminant sensitivity of 0.35, therefore getting an overall poor discriminant efficiency of 0.63. The Common Core of the Pediatric Vocal Symptoms Questionnaire Self-evaluation, Common Core of the Pediatric Vocal Symptoms Questionnaire Parental Evaluation, Common Core of the Pediatric Vocal Symptoms Questionnaire Self-evaluation Reduced version, Common Core of the Pediatric Vocal Symptoms Questionnaire Parental Evaluation Reduced version, Pediatric Vocal Symptoms Questionnaire Self-evaluation Reduced version and Pediatric Vocal Symptoms Questionnaire Parental evaluation Reduced version [20] questionnaires consider a population of children and adolescents aged 6 to 18 years with a diagnosis of dysphonia. All of them aim to measure vocal symptoms in the pediatric population. The first one presents 26 items with the following domains: vocal performance, vocal effort, vocal fatigue, pain symptoms, limitation in vocal activities, phonatory symptoms, and socioemotional symptoms; its cut-off score is 4.45 points. The second presents 20 items, with the domains: vocal performance, vocal effort, vocal fatigue, pain symptoms, and limitation in vocal activities; its cut-off score is 1.45 points. The third presents 10 items, with the same domains as the first one; its cut-off score is 2.75 points. The fourth presents 10 items, with the same domains as the second one described; its cut-off score is 1.75 points. The fifth has 10 items, but no domains; its cut-off score is 2.75 points. The last one presents 15 items without domains; its cut-off score is 1.91 points. As for the response options, all of them present a Likert scale of frequency (never to always), highlighting that the first, third, and fifth questionnaires also present visual support of circles of different sizes from small to very large to assist the response of the child population. The questionnaires Common Core of the Pediatric Vocal Symptoms Questionnaire Parental Evaluation, Common Core of the Pediatric Vocal Symptoms Questionnaire Parental Evaluation Reduced version, and Pediatric Vocal Symptoms Questionnaire Parental evaluation Reduced version [20] are answered by parents or caregivers. The Common Core of the Pediatric Vocal Symptoms Questionnaire Self-evaluation, Common Core of the Pediatric Vocal Symptoms Questionnaire Self-evaluation Reduced version, and Pediatric Vocal Symptoms Questionnaire Self-evaluation Reduce Version [20] are answered by the children and adolescents themselves.
The objective of the study called Development, Validation, and Reliability of the Teacher-Reported Pediatric Voice Handicap Index [21] was to develop a tool to assess pediatric voice from the teachers' perspective and to establish its psychometric properties. This study was conducted in Turkey with 306 father/mother/son/daughter or teacher/child pairs, considering an age range of 4 to 11 years old. The content validity is adequate, being that of the total instrument 0.9, that of the functional domain 0.89, that of the physical domain 0.89, and that of the emotional domain 0.923. The construct validity is high, being 0.96 for the functional domain, 0.94 in the physical domain, and 0.96 in the emotional domain. Criterion validity is low, being 0.65 for the total instrument, 0.47 for the functional domain, 0.68 for the physical domain, and 0.51 for the emotional domain. It presents good internal consistency: 0.98 for the total instrument, 0.94 for the functional domain, 0.96 for the physical domain, and 0.94 for the emotional domain. It has high test-retest reliability, being 0.98 (P<0.001) for the total instrument, 0.91 (P<0.001) for the functional domain, 0.98 (P<0.001) for the physical domain, and 0.96 (P<0.001) for the emotional domain. Finally, sensitivity and specificity yielded a value of P<0.001, indicating significant differences in sensitivity and/or specificity between the groups evaluated. The Teacher-Reported Pediatric Voice Handicap Index (TRPVHI) considers a population of children with dysphonia between 4 and 11 years of age and seeks to measure vocal hand icap in the pediatric population. It presents 27 items with three domains: functional, physical, and emotional, and is answered through a Likert frequency scale (never to always). No cut-off scores are reported in the publication. The questionnaire is answered by teachers of children with dysphonia.
Development and Validation of the Children's Voice Questionnaire (CVQ) [22] aimed to develop and validate the Children's Voice Questionnaire (CVQ), a new self-administered instrument for children. This study was conducted in Turkey with 342 children and adolescents ranging in age from 6 to 18 years. It has a high internal consistency of 0.94. The test-retest reliability was r = 0.79 (P < 0.001), indicating that it is highly reliable. A highly significant difference was observed between the scores of the dysphonic and non-dysphonic groups (t [78,25] = 6.23, P < 0.001). Additionally, there were significant positive correlations of medium to strong strength between children's assessments using the CVQ and their parents' assessments using the pVHI (0.59 < r < 0.66, P < 0.01), indicating strong construct validity. The Children's Voice Questionnaire (CVQ) considers children and adolescents aged 7 to 18 years with a diagnosis of dysphonia and seeks to know the perception of dysphonia and voice-related quality of life. It presents 18 items without the presence of domains and is answered through a Likert frequency scale (never to always). Its cut-off scores for the control group are 4.2 (+-5.58) points and for the experimental group, 14.66 (+-14.06) points. The questionnaire is answered by the children and adolescents themselves.
Discussion
The term "self-assessment questionnaires" may seem somewhat contradictory when it comes to assessing the pediatric population since they aim to understand the patient's own perception of himself/herself [24]. However, despite collecting information on the health, symptoms, and quality of life of a child, in most cases these tools are completed by third parties, fulfilling a role of informants of relevant data on the symptomatology of infants. Most of the pediatric vocal self-assessment questionnaires that were found in this review are answered by parents, guardians, caregivers, or teachers; therefore, it moves away from the main purpose of the questionnaire which is to know the repercussions of pediatric dysphonia in different spheres of daily life from one's perspective. The answers provided by children are reliable about their dysphonia and quality of life if the assessment is designed specifically for them [22]. Therefore, when creating and implementing self-assessment questionnaires, the limitations and capabilities of the child population to solve the tools autonomously should be considered.
One of the articles that was excluded in this review, according to the methodological process, was the one named Cut-off point for high dysphonia risk in children based on the Child Dysphonia Risk Screening Protocol: preliminary findings [25], which aims to establish cut-off scores for a questionnaire already created previously, called Child Dysphonia Risk Screening Protocol (DRSP-C). Unfortunately, no publication of the scientific article describing the original creation of this questionnaire was found in the databases consulted. A search using a narrative review (outside the search criteria established in advance) found an abstract presented at the 42nd symposium of The Voice Foundation titled Proposal for pediatric population dysphonic screening protocol [26], in which an adapted version of the Dysphonia risk screening protocol , called Child Dysphonia Risk Screening Protocol, is presented for the pediatric voice. This questionnaire is answered by the responsible adult, contains 14 items related to vocal behavior, and is answered using a Likert frequency response scale with the options always, sometimes, never or I don't know. Despite being qualified as a good evaluation instrument in the pediatric population, since it seeks to detect vocal disorders related to vocal behavior in the child population [25], it was not possible to include it in the present review due to the aforementioned.
It is important to highlight that in the study entitled Development and validation of a short version of the Spanish pediatric voice handicap index (P-VHI-10) [20] an abbreviated version of the Pediatric Voice Handicap Index [13] was made, considering for its construction the 10 items with the highest scores for the Spanish validated version of the P-VHI, originating the Spanish pediatric voice handicap index (P-VHI-10); In addition, he used the questionnaire created in Italy, but translated into English Children's Voice Handicap Index-10, to create a Spanish version to be answered by parents, called with the abbreviation C*-VHI-10, without indicating the full name of the tool. This creation was not considered for this scope review because it was an adaptation made from the C-VHI-10 translated into English, that is, the adaptation was not made from the original version in Italian, failing to comply with the established methodological criteria, since in the development of questionnaire validation it is essential to start this process in the original language and it must be confirmed that the structure is not altered when the language is changed [27]. In addition, despite being mentioned in the methods of the document, the methodology for the creation of this tool is not described in detail, so it could not be included.
The article called Development and Validation of the Children's Voice Questionnaire (CVQ) [22] presents the original Hebrew language creation of the Children's Voice Questionnaire (CVQ), as well as its English version. This English version followed and detailed a neat methodology, considering bidirectional translation, which serves as a tool that facilitates obtaining comprehensible information in two different linguistic systems, allowing to processing of meanings mutually [28]. Considering that one of the languages included in the search was English, due to the above-mentioned, this questionnaire could be included in the research since both versions are exposed in the same article and the methodological process of linguistic adaptation carried out is indicated in detail.
Of the 12 articles included in this review, it is evident that 3 of them presented a sample of less than 100 people, which could generate biases or inaccurate results in the research since they would be less representative of the population studied [29]. Another point to note about the sample is the heterogeneity of the age range, because the concept of child involves any person up to 14 years of age [30] and some samples in the research reviewed cover ages from 0 to 14 years, as well as others that include ages from 0 to 21 years, which generates contradiction, as they should not be called pediatric questionnaires if they include ages that are considered outside the child age range.
To ensure that valid and reliable information is obtained and to guarantee meaningful assessment results, it is important to have robust psychometric measures of the instruments [31]. Establishing the psychometric measures for an instrument to be valid will depend on the author's vision. For example, some say that it should be composed of reproducibility, validity, sensitivity, and usefulness [32], while others propose the methodological sequence composed of reliability, internal consistency, stability, equivalence, and validity, to reduce biases in the interpretation of the results [33]. These properties need to be examined in each measurement test, to verify that they are calibrated and that they meet the study objectives to be used [34]. From the results analyzed, most of the selected questionnaires comply with the same psychometric measures, such as validity, sensitivity, specificity, and reliability. However, in the text Glottal Function Index: A Predictor of Glottal Disorders in Children [14] only the sensitivity and specificity are indicated, but the results report that the questionnaire is reliable. The Pediatric Voice Handicap Index (pVHI): A new tool for evaluating pediatric dysphonia [13] is based on quantifying internal consistency and reliability, thus not mentioning other measurement variables; despite this, it is still a reliable questionnaire for the pediatric population. Therefore, there is uncertainty as to how many of these parameters are necessary to consider an instrument valid and reliable, since these properties vary both in the literature and the various studies.
Conclusions
Pediatric vocal self-assessment questionnaires are necessary tools for vocal evaluation, as they provide a personal view on emotional, functional, and physical aspects, symptomatology, and quality of life perceived by the child or adolescent. Due to this, the study focused on describing the pediatric vocal self-assessment instruments created worldwide and, in this context, the objectives were met since 17 original pediatric vocal self-assessment questionnaires were identified and described.
The limitation identified in this study was to search only the Scopus, SciELO, WOS, and PubMed databases, excluding the gray literature, which could have provided information on questionnaires not found in the search engines.
This review aims to contribute to the field of speech-language pathology in the vocal area by providing a mapping and description of existing pediatric vocal self-assessment questionnaires and their respective characteristics. It is recommended to use the information of this review to facilitate therapeutic decision-making so that the speech-language pathologist can select and implement the most suitable questionnaire for each individual requirement.
Based on these findings, it is hoped that future research can analyze which of the described questionnaires have been adapted and culturally validated for use in different countries.
References
1. Gómez Sánchez V. Estudio de la vulnerabilidad de la voz en niños de 8 y 10 años con disfonía infantil [bachelor’s thesis]. [Cantabria]: Universidad de Cantabria; 2015. 27 p. Available from: http://hdl.handle.net/10902/15618
2. Fleta Zaragozano J. Disfonía en la infancia. Valoración y pauta a seguir. Boletín de la Sociedad de Pediatría de Aragón, La Rioja y Soria [Internet]. 2021;51(2): 81-5. Available from: https://dialnet.unirioja.es/servlet/articulo?codigo=8098046
3. Antón Almero M, Reig Montaner E, Ferrer Ramírez MJ, Doménech Máñez I, Huerta Barberá S, Revenga Nieto G. D. Impacto de la disfonía en la calidad de vida en la edad infantil. Revista de Logopedia, Foniatría y Audiología [Internet]. 2022;42(4): 208-13. doi: https://doi.org/10.1016/j.rlfa.2021.02.005
4. Alcaíno Navarrete VP, Bobadilla Mellado PA, Cortés Arellano VE, Pozo Bustamante AA. Cuestionarios que evalúan la calidad de vida relacionada con disfonía en población pediátrica: una revisión sistemática. [bachelor's tesis]. Talca: Universidad de Talca; 2020. 53 p. Available from: http://dspace.utalca.cl/handle/1950/12880
5. Centeno D, Nercelles L, Valenzuela J, Catalán C. Análisis descriptivo del índice de discapacidad vocal pediátrico en niños con patología vocal benigna. Rev Otorrinolaringol Cir Cabeza Cuello [Internet]. 2022;82(1):16-20. doi: https://doi.org/10.4067/s0718-48162022000100016
6. Malebrán MC, Henríquez L, Contreras-Ruston F. Revisión narrativa de instrumentos de autoevaluación vocal en Chile. Rev Otorrinolaringol Cir Cabeza Cuello [Internet]. 2021;81(4):615-21. doi: https://doi.org/10.4067/s0718-48162021000400615
7. Inostroza-Moreno G. Orientaciones filosóficas en la intervención fonoaudiológica de voz. El desafío actual de dar el alta. Rev Investig Innov Cienc Salud [Internet]. 2021;3(1):116-24. doi: https://doi.org/10.46634/riics.34
8. Chambergo-Michilot D, Diaz-Barrera ME, Benites-Zapata VA. Revisiones de alcance, revisiones paraguas y síntesis enfocada en revisión de mapas: aspectos metodológicos y aplicaciones. Rev Peru Med Exp Salud Publica [Internet]. 2021;38:136-42. doi: https://doi.org/10.17843/rpmesp.2021.381.6501
9. Grant M, Brooth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J [Internet]. 2009;26(2):91-108. doi: https://doi.org/10.1111/j.1471-1842.2009.00848.x
10. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ [Internet]. 2021;372:n71. doi: https://doi.org/10.1136/bmj.n71
11. Hartnick CJ. Validation of a pediatric voice quality-of-life instrument: the pediatric voice outcome survey. Arch Otolaryngol Head Neck Surg [Internet]. 2002;128(8):919-22. doi: https://doi.org/10.1001/archotol.128.8.919
12. Boseley ME, Cunningham MJ, Volk MS, Hartnick CJ. Validation of the pediatric voice-related quality-of-life survey. Arch Otolaryngol Head Neck Surg [Internet]. 2006;132(7):717-20. doi: https://doi.org/10.1001/archotol.132.7.717
13. Zur KB, Cotton S, Kelchner L, Baker S, Weinrich B, Lee L. Pediatric Voice Handicap Index (pVHI): a new tool for evaluating pediatric dysphonia. Int J Pediatr Otorhinolaryngol [Internet]. 2007;71(1):77-82. doi: https://doi.org/10.1016/j.ijporl.2006.09.004
14. Cohen JT, Oestreicher-Kedem Y, Fliss DM, DeRowe A. Glottal function index: a predictor of glottal disorders in children. Ann Otol Rhinol Laryngol [Internet]. 2007;116(2):81-4. doi: https://doi.org/10.1177/000348940711600201
15. Verduyckt I, Morsomme D, Remacle M. Validation and standardization of the Pediatric Voice Symptom Questionnaire: a double-form questionnaire for dysphonic children and their parents. J Voice [Internet]. 2012;26(4):e129-e139. doi: https://doi.org/10.1016/j.jvoice.2011.08.001
16. Ricci-Maccarini A, De Maio V, Murry T, Schindler A. Development and validation of the children's voice handicap index-10 (CVHI-10). J Voice [Internet]. 2013;27(2):258.e23-258.e28. doi: https://doi.org/10.1016/j.jvoice.2012.10.006
17. Ricci-Maccarini A, De Maio V, Murry T, Schindler A. Development and validation of the Children's Voice Handicap Index-10 for parents. J Voice [Internet]. 2016;30(1):120-6. doi: https://doi.org/10.1016/j.jvoice.2014.10.004
18. Cohen W, Wynne DM. Parent and child responses to the pediatric voice-related quality-of-life questionnaire. J Voice [Internet]. 2015;29(3):299-303. doi: https://doi.org/10.1016/j.jvoice.2014.08.004
19. Sanz L, Bau P, Arribas I, Rivera T. Development and validation of a short version of the Spanish pediatric voice handicap index (P-VHI-10). Int J Pediatr Otorhinolaryngol [Internet]. 2016;88:113-6. doi: https://doi.org/10.1016/j.ijporl.2016.06.053
20. Lima L, Behlau M. Pediatric Vocal Symptoms Questionnaire (PVSQ): Four new versions for parental evaluation and self-evaluation. Int J Pediatr Otorhinolaryngol [Internet]. 2020;131:109816. doi: https://doi.org/10.1016/j.ijporl.2019.109816
21. Yağcıoğlu D, Aydınlı FE, Aslan G, Kirazlı MÇ, Köse A, Doğan N. Development, Validation, and Reliability of the Teacher-Reported Pediatric Voice Handicap Index. Lang Speech Hear Serv Sch [Internet]. 2022;53(1):69-87. doi: https://doi.org/10.1044/2021_LSHSS-21-00033
22. Amir O, Bar-David OY, Goldstein S, Epstein R, Alston M, Roziner I, et al. Development and Validation of the Children’s Voice Questionnaire (CVQ). J Voice [Internet]. Forthcoming 2023 Oct 31. doi: https://doi.org/10.1016/j.jvoice.2023.09.030
23. Bach KK, Belafsky PC, Wasylik K, Postma GN, Koufman JA. Validity and reliability of the glottal function index. Arch Otolaryngol Head Neck Surg [Internet]. 2005;131(11):961-4. doi: https://doi.org/10.1001/archotol.131.11.961
24. Crevier Buchman L, Mattei A, Giovanni A. Uso forzado de la voz. EMC-Otorrinolaringología [Internet]. 2020;49(1):1-16. doi: https://doi.org/10.1016/S1632-3475(19)43324-9
25. Batista GKS, Simões-Zenari M, Nemr K. Cut-off point for high dysphonia risk in children based on the Child Dysphonia Risk Screening Protocol: preliminary findings. Clinics (Sao Paulo) [Internet]. 2020;75:e1682. doi: https://doi.org/10.6061/clinics/2020/e1682
26. Nemr NK, Simões-Zenari M, Lobrigate KE. Proposal for pediatric population dysphonic screening protocol. 42nd Annual Symposium: Care of the Professional Voice; 2013 May 29 - Jun 2; Philadelphia: The Voice Foundation.
27. Carvajal A, Centeno C, Watson R, Martínez M, Sanz Rubiales Á. ¿Cómo validar un instrumento de medida de la salud? An sist sanit Navar [Internet]. 2011;34(1):63-72. doi: https://doi.org/10.4321/S1137-66272011000100007
28. Jiménez González MA, Aguilera Ramírez M, Morales Vázquez E. El aprendizaje de Inglés como Segunda Lengua mediante la traducción bidireccional. Cienc lat [Internet]. 2023;7(2):3594-619. doi: https://doi.org/10.37811/cl_rcm.v7i2.5601
29. Manterola C, Otzen T. Porqué investigar y cómo conducir una investigación. Int J Morphol [Internet]. 2013;31(4):1498-504. doi: https://doi.org/10.4067/S0717-95022013000400056
30. Ministerio de Desarrollo Social y Familia de Chile, Subsecretaría de la Niñez de Chile. Guía Didáctica para la Ley 21.430. Sobre Garantías y Protección Integral de los Derechos de la Niñez y Adolescencia. The World Bank; 2022, 76 p.
31. Valdés Cuervo ÁA, Carlos Martínez EA, Vera Noriega JÁ, Montoya Verdugo G. Propiedades psicométricas de un instrumento para medir las relaciones familiares en adolescentes intelectualmente sobresalientes. Pensam psicol [Internet]. 2012;10(1), 39-50. Available from: https://revistas.javerianacali.edu.co/index.php/pensamientopsicologico/article/view/209
32. Luján Tangarife JA, Cardona Arias JA. Construcción y validación de escalas de medición en salud: revisión de propiedades psicométricas. Archivos de Medicina [Internet]. 2015;11(3):1-10. Available from: https://www.itmedicalteam.pl/articles/construccin-y-validacin-de-escalasde-medicin-en-salud-revisin-depropiedades-psicomtricas-103291.html
33. Argibay JC. Técnicas psicométricas. Cuestiones de validez y confiabilidad. Subj procesos cogn [Internet]. 2006;(8):15-33. Available from: http://dspace.uces.edu.ar:8180/xmlui/handle/123456789/765
34. Rosario-Rodríguez A, Rodríguez-Montalbán R, Martínez-Lugo M. Propiedades psicométricas de la Escala de Comportamientos de Ciudadanía Organizacional (ECCO). Rev Puertorriquena Psicol [Internet]. 2019;30(1):30-46. Available from: https://www.repsasppr.net/index.php/reps/article/view/393
Appendix. Database Search.
Figure A. Search in PubMed database.
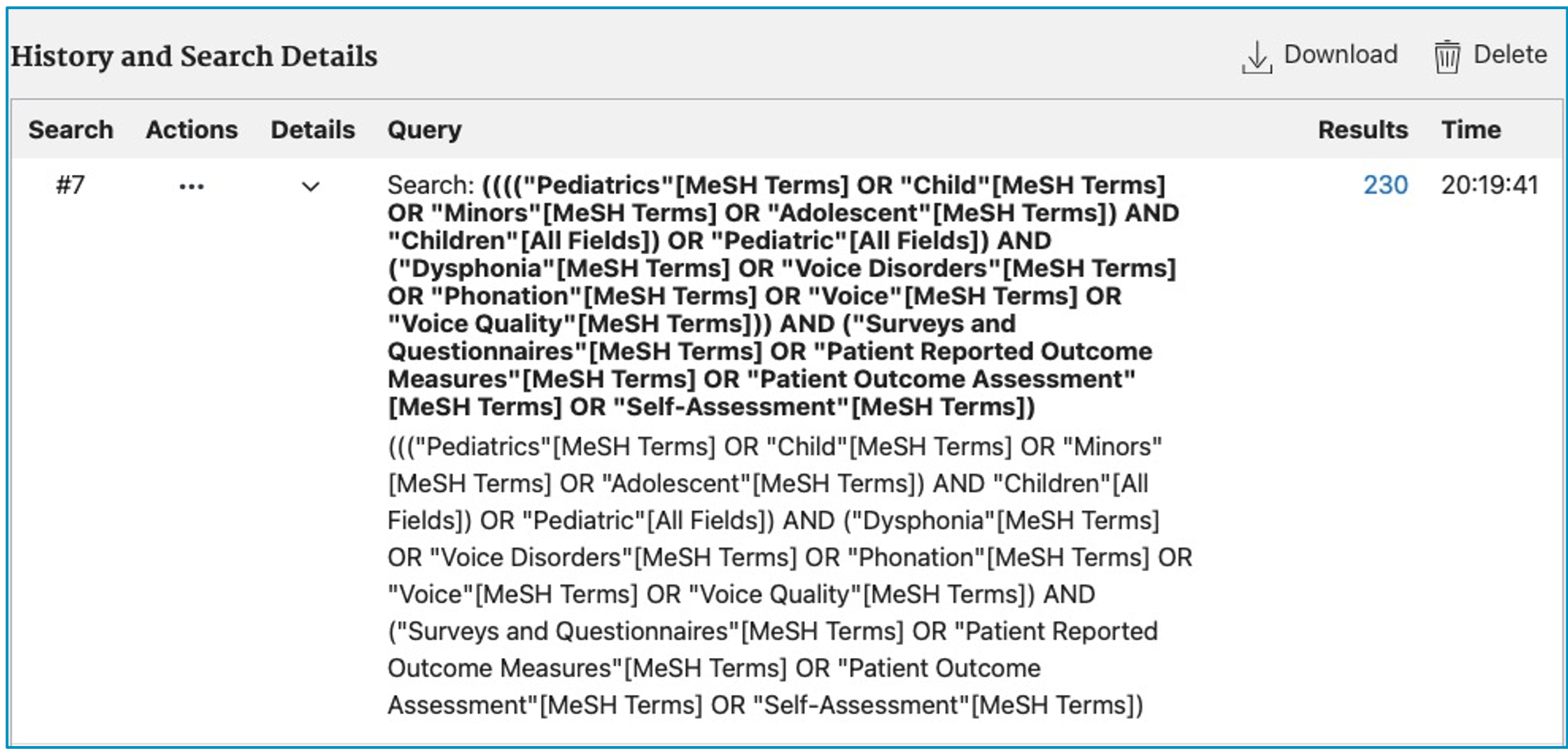
Figure B. Search in Scopus database.

Figure C. Search in SciELO database.

Figure D. Search in WOS database.