
Self-reported Effects of Vocal Health Promotion Videos on Teachers
Efecto autoinformado de los videos de promoción de la salud vocal en docentes
Abstract
Introduction. Guidance on vocal health promotion can benefit teachers; however, the impact of presenting such guidance in videos is not well understood.
Objective. To evaluate the self-reported effects of vocal health promotion videos on a cohort of teachers.
Method. Cross-sectional observational study. Two videos containing speech therapy guidance for voice management in both remote and resuming in-person classes during the COVID-19 pandemic were distributed to 1081 teachers. Subsequently, an online questionnaire was administered to the teachers to assess their learning from the videos, changes in vocal habits resulting from the content, specific behavioral changes, and suggestions for additional health promotion initiatives. Descriptive and inferential analyses were performed using the Mann-Whitney U test and Fisher's exact test.
Results. Thirty-three teachers participated in the study. Participants positively evaluated the videos and reported implementing changes in their vocal habits and teaching practices. They also noted post-viewing improvements in their voices. Changes in behavior included reduced smoking, increased water intake, decreased shouting and throat clearing, improved relaxation and reduced tension during classes, and improved eating habits. Most teachers indicated that remote speech therapy guidance was more accessible than in-person consultations.
Conclusion. The videos promoted self-perception and facilitated positive changes, improving the teachers’ vocal health and communication.
Keywords
Voice; voice disorders; voice training; speech therapy; school teachers; faculty; occupational health; health education; health promotion; COVID-19.
Resumen
Introducción. La orientación sobre la promoción de la salud vocal puede ser beneficiosa para los profesores. Sin embargo, el impacto de presentar dicha orientación en formato de video no está bien comprendido.
Objetivo. Evaluar los efectos autorreportados de videos de promoción de la salud vocal en un grupo de profesores.
Método. Estudio observacional transversal. Se distribuyeron dos videos con orientación de terapia del habla para el manejo de la voz en clases remotas y el retorno presencial durante la pandemia de Covid-19 a 1081 profesores. Posteriormente, se administró un cuestionario en línea a los profesores para evaluar su aprendizaje de los videos, cambios en hábitos vocales como resultado del contenido, comportamientos específicos modificados y sugerencias para iniciativas adicionales de promoción de la salud. Se realizaron análisis descriptivos e inferenciales utilizando la prueba U de Mann-Whitney y la prueba exacta de Fisher.
Resultados. Treinta y tres profesores participaron en el estudio. Los participantes proporcionaron evaluaciones positivas de los videos y reportaron implementar cambios tanto en sus hábitos vocales como en sus prácticas de enseñanza. Además, notaron mejoras en sus voces después de ver los videos. Los cambios en el comportamiento incluyeron la reducción del tabaquismo, aumento en la ingesta de agua, disminución en gritos y aclaraciones de garganta, mejora en la relajación y reducción de la tensión durante las clases y hábitos alimenticios mejorados. La mayoría de los profesores indicaron que la orientación remota de terapia del habla era más accesible en comparación con las consultas presenciales.
Conclusiones. Los videos fomentaron la autopercepción y facilitaron cambios positivos, resultando en una mejor salud vocal y comunicación entre los profesores.
Palabras clave
Voz; trastornos de la voz; entrenamiento de la voz; logopedia; maestros; docentes; salud laboral; educación en salud; promoción de la salud; COVID-19.
Introduction
Voice disorders are more prevalent among teachers than non-teachers. Between 51.2% and 63% of teachers have experienced some form of vocal impairment at some point in their careers [1,2]. In addition, teachers have more vocal symptoms and report occupational voice limitations more often, such as tired or changing vocal quality after short use, difficult voice projection, vocal discomfort, and increased effort to talk [1]. Voice disorders limit work-related activities, increase absenteeism, and are the main reason teachers leave their occupations [3]. Hence, attention should be drawn to their economic impact not only on teachers but also on society.
Moreover, dysphonia adversely affects these workers’ quality of life since the voice is the main tool of their trade, and their performance and day-to-day activities depend on it [4]. A study showed that children have difficulty understanding the content presented by teachers with hoarse voices, whether in a formal assessment or a noisy classroom, indicating that a dysphonic voice can compromise the result of pedagogical activities [5]. Therefore, voice disorders have significant economic, occupational, personal, and social impacts on teachers, highlighting the need for actions to prevent dysphonia among them.
This has challenged specialists and researchers for decades, particularly speech therapists. The COVID-19 pandemic, caused by the new coronavirus, changed the teaching process and raised questions about such changes. Research has found that, although most teachers noticed improvement in their voices, some who worked remotely reported their voices worsened during the pandemic [6] with stress-related impacts [7,8]. This was seen mainly among teachers with more years of experience since they are more used to the conditions of the face-to-face work environment. The main difficulties reported with remote classes were hoarseness, vocal fatigue, dissatisfaction with vocal quality, voice failures, sore throat, dry throat, throat clearing, and difficulty with technology [6]. There is evidence that these symptoms may be related to psychological stress caused by the transition to remote classes and adaptation to the new working environment with different sound reverberation characteristics and ways of teaching [6-8].
Teachers were required to reorganize and adapt to the dynamics, space, and specificities of emergency remote teaching during the pandemic. These changes require the health professionals’ guidance and care for teachers to minimize the impacts of the pandemic.
There is evidence that actions to promote vocal health and prevent voice disorders have results, regardless of the presence of voice disorders. Thus, implementing everyday beneficial vocal habits and reducing harmful ones reduce vocal symptoms and stress and improve vocal and communicative performance, positively impacting quality of life and other aspects [9,10]. Similar results have been observed in remote [11] and blended (both in-person and remote) activities [12], and studies aimed at changing vocal habits and training the voice usually show more significant results. Thus, we hypothesized that the guidelines in two vocal health promotion videos would stimulate self-perception and facilitate changes, positively impacting the voice and communication of the teachers who watched them.
Therefore, this study aimed to evaluate the self-reported effects of vocal health promotion videos on teachers.
Method
Study design
Cross-sectional observational research, with the approval of the institution's ethics committee.
The sample comprised Brazilian teachers from various educational levels and disciplines who had participated in previous research [6] and received informational voice and communication material during the COVID-19 pandemic via email. Figure 1 presents the participants’ flowchart.
Figure 1. Flowchart of the participants.
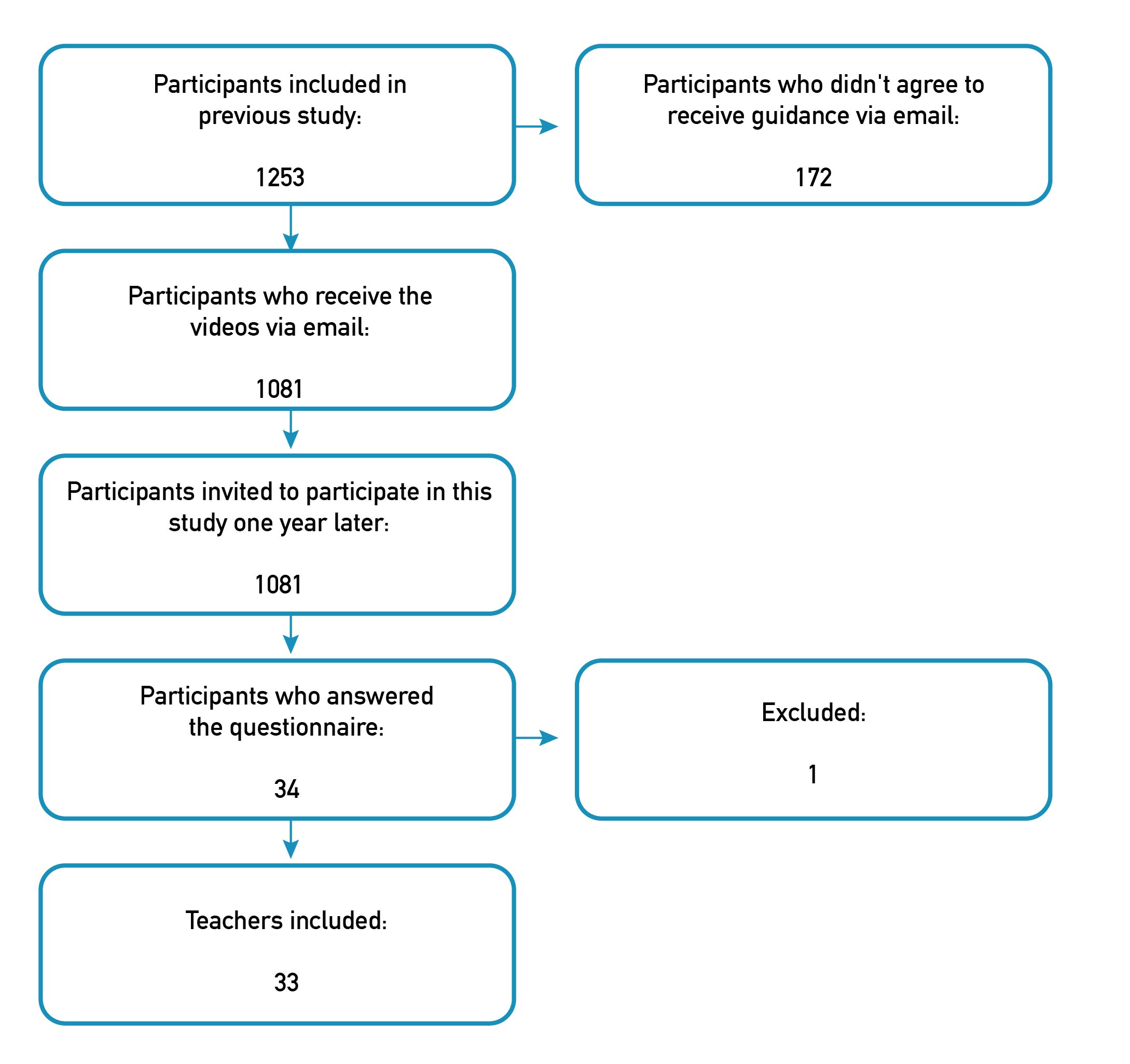
Inclusion criteria were having participated in the previous study and agreeing to receive informational materials by email.
Exclusion criteria were answering the questionnaire incompletely, duplicate questionnaires, and not having watched at least one of the videos in question.
Videos
A previous study that aimed to understand the effects of changes at work -resulting from the COVID-19 pandemic- on teachers’ voices included teachers from all Brazilian regions, working at different education levels and institutions [6]. Thus, after concluding the study, two videos were produced - “Teacher's Voice - Part 1” and “Teacher's Voice - Part 2” -, made available on YouTube, and sent to interested participants via email. This action aimed to guide teachers on voice use during remote and blended work -as in-person classes (wearing face masks) resumed in Brazil at a certain point in the pandemic, simultaneously with remote activities.
Videos 1 and 2 were prepared in Portuguese and sent to teachers via email in September 2020 and June 2021, respectively. Both are freely available on YouTube: https://youtu.be/kZQc7GbJ1X4 (Video 1) and https://youtu.be/_0hbdETwhjI (Video 2).
Video 1. Teacher's Voice - Part 1.
Note. The rights to the video belong to and remain with LIFVoz. The journal has obtained authorization for its publication.
Video 2. Teacher's Voice - Part 2.
Note. The rights to the video belong to and remain with LIFVoz. The journal has obtained authorization for its publication.
The videos were developed based on the main difficulties pointed out by the teachers in the first study and on topics already covered in other studies in the literature. The videos are animations with a narrator explaining each topic. Video 1 lasts seven minutes and addresses teacher communication in in-person and remote classes, emphasizing topics such as vocal production, vocal hygiene, expressiveness, and environmental factors, including workplace ergonomics. Video 2, in turn, lasts eleven minutes and focuses on resuming in-person and blended classes (in which some students attended classes in person, while others remained online) and provides guidance on vocal use with a face mask and care when returning to school after having contracted COVID-19.
Questionnaire
The authors prepared the questionnaire for this research on Google Forms, which is easy for participants to access and handle. The questionnaire (available in the supplementary material) had 60 questions and took about 10-15 minutes to complete.
The first questions surveyed which video(s) (Video 1 and Video 2) the participating teacher had watched, and then asked for their sociodemographic data. In the next section, teachers were required to score from 0 to 10 (0 being the worst score -it did not help me at all- and 10 being the best score -it helped me a lot) their perception of the help provided by the videos at different times of teaching practice during the pandemic: during remote classes, resuming in-person classes, and currently (as they answered the questionnaire). They were also asked to score the application of the guidelines in their daily lives, considering 0 as the worst score (I have not applied anything) and 10 as the best score (I have applied the guidance completely). Thus, the higher the score on these questions, the better the teachers’ evaluation.
In the following section, participants answered yes/no and open questions regarding the changes they made following the guidance in the videos. Then, they evaluated whether they agreed or disagreed with some statements related to voice, vocal health, and communication regarding the period before and after watching the videos. These questions were based on the guidelines in Videos 1 and 2.
The last section had some optional additional information, with open questions for participants to suggest improvements to the guidelines and the means of access they deemed more viable to receive the guidelines. This final section was analyzed qualitatively, based on the video topics.
The questionnaire was administered remotely in August and September 2022. An invitation to participate, containing the research objectives and the link to access the questionnaire, was emailed to the teachers who had access to the informative material. They could rewatch the videos and were instructed to answer the questionnaire with their perceptions of the help provided by the videos. The research did not focus on a longitudinal evaluation but on the self-reported impact after the action. In total, three reminders were sent to the participants to complete the questionnaire. However, as the only means of communication available was via email, a considerable number of teachers may not have seen the message, which influenced the number of responses.
Study participants
The study included 33 teachers, of whom 33 (100%) watched Video 1, while 90.91% (n = 30) watched Video 2, -i.e., three participants (9.09%) did not watch the second video.
Among the participants, 24 were females (72.73%) and nine were males (27.27%), aged 31 to 64 years, with a mean of 50 years. Their teaching experience ranged from 4 to 42 years, with a mean of 20.79 years. Also, 15.15% (n = 5) taught from nursery school to kindergarten, 30.30% (n = 10) in elementary school, 24.24% (n = 8) in middle school, 30.30% (n = 10) in high school, 21.21% (n = 7) in higher education, and 12.12% (n = 4) in private courses/classes -10 teachers (30.30%) worked in more than one education level or type. Moreover, 93.94% (n = 31) of the teachers lived in Southeastern Brazil and worked in the capital of their state, where socioeconomic conditions are better.
Concerning their voices, 36.36% (n = 12) reported having had vocal problems before the pandemic: three cited vocal nodules, seven cited vocal symptoms (especially hoarseness and dry throat), one cited glottal gap, and one cited vocal fold cyst. Three participants (9.09%) reported having taken leaves of absence two to four times due to voice problems. Five teachers (15.15%) had previously attended or were currently attending speech therapy for the voice.
Data analysis
After receiving the completed questionnaires, the data were arranged in an Excel spreadsheet to analyze the results. Descriptive and inferential analyses were performed using SPSS Statistics software, version 28.0 (IBM Corp., Armonk, NY, USA).
The descriptive analysis considered the measures of central tendency and dispersion. The inferential analysis assessed the association between having and not having prior knowledge about voice production and perceiving changes in voice and communication for the worse, the better, or no changes after the videos, as well as before the videos and after them. In questions whose answer options were agree, partially agree, and disagree, the researchers joined agree and partially agree into one for greater statistical analysis power, leaving only two options: agree or disagree. The Mann-Whitney U test (for ordinal qualitative variables) and Fisher's exact test (for nominal qualitative variables) were used for the inferential analysis. The statistical significance was set at 5% (p ≤ 0.05).
The results are presented according to the questionnaire sections.
Results
Evaluation of the videos
Table 1 presents the scores awarded by the teachers for the help provided by the videos at different times in their teaching practice during the pandemic and for applying the guidelines in their daily lives. The mean scores were above 7 points to the help provided by videos during different moments of the pandemic.
Table 1. Scores given by teachers on the contribution of the videos.
| Question | Mean | SD | Median | Min. | Max. |
|---|---|---|---|---|---|
| How much did the videos help you during remote classes? | 7.39 | 2.81 | 8.00 | 0.00 | 10.00 |
| How much did the videos help as in-person classes resumed? | 7.27 | 2.99 | 8.00 | 0.00 | 10.00 |
| How much are the videos helping you right now? | 7.70 | 2.28 | 8.00 | 0.00 | 10.00 |
| How much have you applied the guidelines in your professional day-to-day activities? | 7.15 | 2.45 | 8.00 | 0.00 | 10.00 |
Note. SD: Standard deviation; Min.: Minimum; Max.: Maximum.
Changes after watching the videos
Teachers were asked about the changes they made in different areas involving their professional day-to-day activities after watching the videos. Figure 2 presents the percentages of participants who changed and did not change their vocal habits, work environment, and teaching practice.
Figure 2. Comparison between making and not making changes in professional day-to-day activities per area.
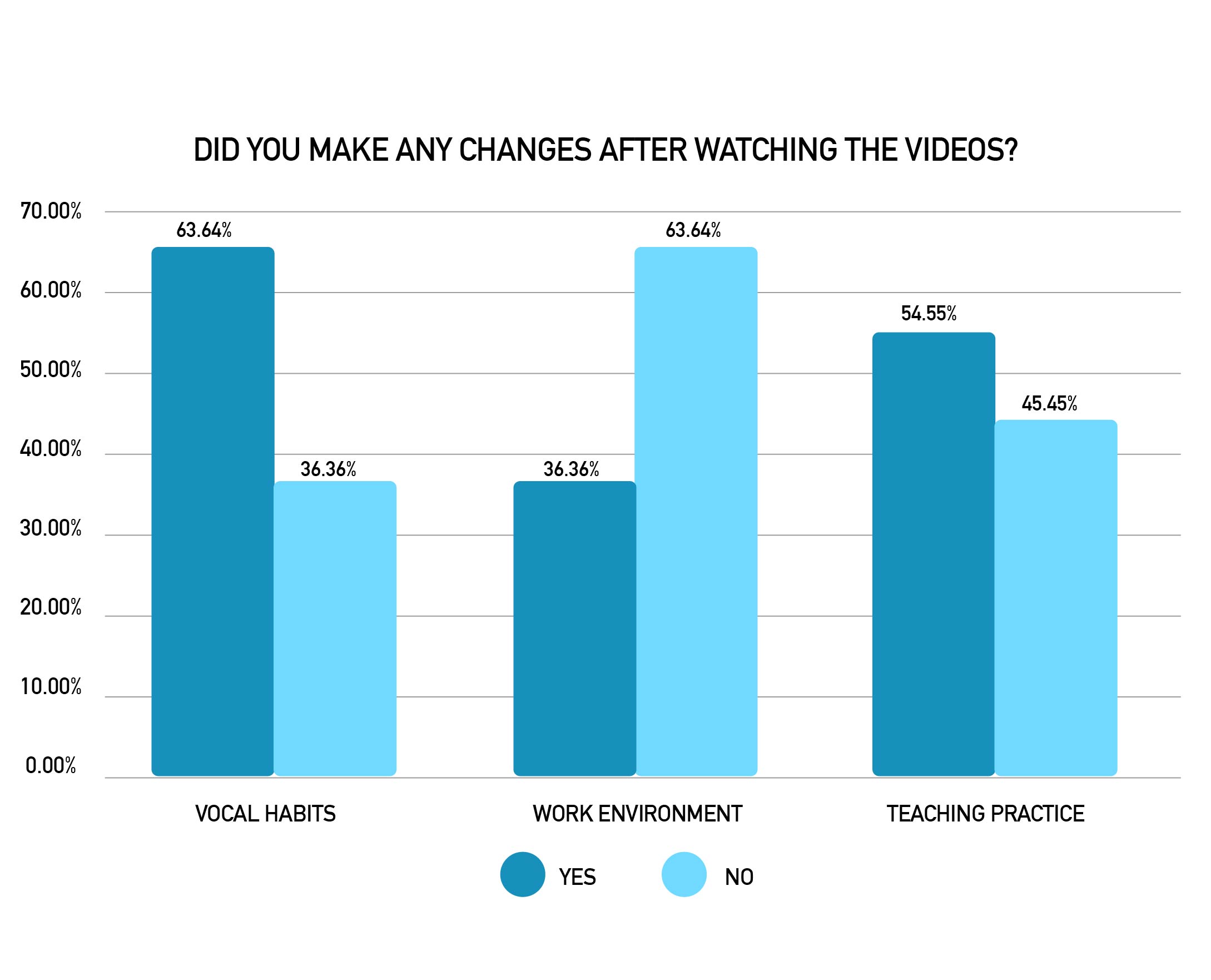
Participants who reported making changes could describe what they had changed, and this was arranged in a list from the most to the least cited. Regarding vocal habits, the teachers mentioned increased water intake, reduced vocal intensity, attention to body posture, taking more breaks during speech, performing vocal exercises, and so forth. Regarding the work environment, teachers reported including noise reduction strategies, improving the screen position in remote and blended classes, changing the room organization, improving the workspace ventilation, and so on. Concerning teaching practice strategies, they mentioned the use of active tools and methodologies, making agreements with students to avoid speaking loudly, using a microphone, paying attention to their position in relation to students during communication, drinking water during class, and so on.
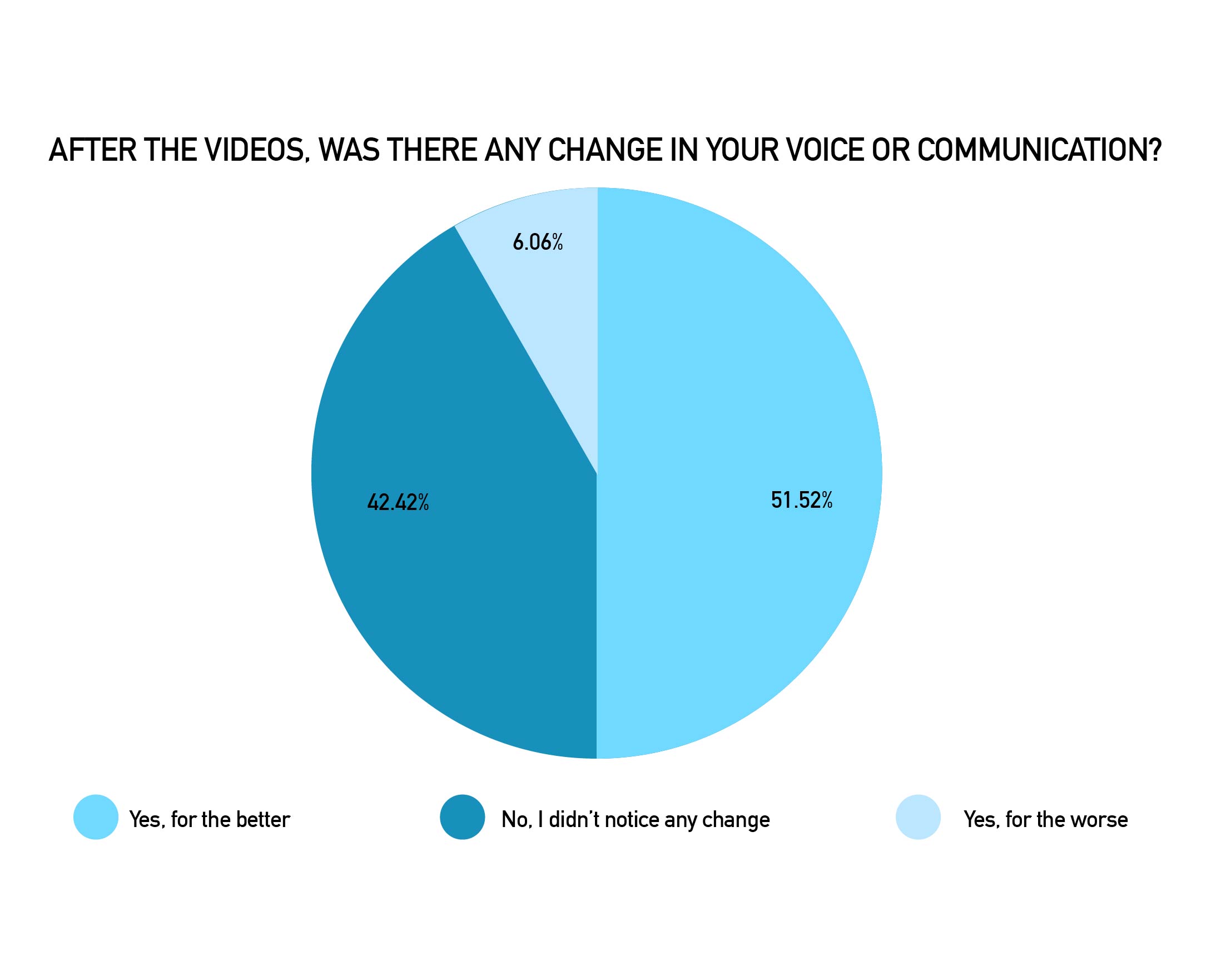
Teachers were also asked if they had noticed any changes in their voices and communication after watching the videos, most of whom reported improvements (Figure 3).
Figure 3. Number of teachers who noticed or did not notice any change in their voices or communication after watching the videos.
The individuals were compared in terms of having or not having prior knowledge about voice production and reporting voice and communication changes after the videos. According to Fisher's exact test, there was no significant difference (Table 2).
Table 2. Comparison of teachers with and without prior knowledge according to changes in voice and communication after the videos.
| Before the videos, I had little or no knowledge of voice production | ||||||||
|---|---|---|---|---|---|---|---|---|
| Category | Disagree | Agree | Total | p | ||||
| n | % | n | % | n | % | |||
| Have there been any changes in your voice and communication? | Yes, for the worse | 2 | 12.50 | 0 | 0.00 | 2 | 6.07 | 0.368 |
| No, I didn't notice any changes | 7 | 43.75 | 7 | 41.18 | 14 | 42.42 | ||
| Yes, for the better | 7 | 43.75 | 10 | 58.82 | 17 | 51.51 | ||
Note. Fisher's exact test.
Behaviors before and after watching the videos
The questionnaire had statements regarding before and after viewing the videos, and the teachers were asked to indicate whether they agreed with these statements. Tables 3, 4 and 5 compare teachers regarding their behavior before and after the videos. Fisher's exact test demonstrated that they had changed behaviors such as smoking, consuming alcoholic beverages, being relaxed without body tension during classes, increasing daily water intake, having an adequate diet, and decreasing the habit of shouting and clearing their throats.
Table 3. Comparison of teachers according to behavior in relation to behavioral changes after the videos.
| Behavior before watching the videos | ||||||||
|---|---|---|---|---|---|---|---|---|
| Behavior after watching the videos | Category | Before the videos, I had little or no knowledge of voice production | ||||||
| Disagree | Agree | Total | p | |||||
| n | % | n | % | n | % | |||
| After watching the videos, I understood better how my voice is produced | Disagree | 2 | 12.50 | 0 | 0.00 | 2 | 6.06 | 0.227 |
| Agree | 14 | 87.50 | 17 | 100 | 31 | 93.94 | ||
| Before watching the videos, I smoked | ||||||||
| After watching the videos, I tried to reduce smoking | Disagree | 0 | 0.00 | 1 | 50.00 | 1 | 3.03 | 0.002* |
| Agree | 0 | 0.00 | 1 | 50.00 | 1 | 3.03 | ||
| Not applicable | 31 | 100.00 | 0 | 0.00 | 31 | 93.94 | ||
| Before watching the videos, I consumed alcohol | ||||||||
| After watching the videos, I tried to reduce alcohol consumption | Disagree | 0 | 0.00 | 9 | 90.00 | 9 | 27.27 | < 0.001* |
| Agree | 0 | 0.00 | 1 | 10.00 | 1 | 3.03 | ||
| Not applicable | 23 | 100.00 | 0 | 0.00 | 23 | 69.70 | ||
| Before watching the videos, I hadn't thought about the importance of sleep | ||||||||
| After watching the videos, I understood the importance of quality sleep and searched for strategies to sleep better | Disagree | 5 | 33.33 | 2 | 11.11 | 7 | 21.21 | 0.203 |
| Agree | 10 | 66.67 | 16 | 88.89 | 26 | 78.79 | ||
| Before watching the videos, I didn't take care of my general health | ||||||||
| After watching the videos, I started to take more care of my general health | Disagree | 7 | 35.00 | 1 | 7.69 | 8 | 24.24 | 0.108 |
| Agree | 13 | 65.00 | 12 | 92.31 | 25 | 75.76 | ||
| Before watching the videos, I had not thought about the importance of being relaxed and free of body tension during classes | ||||||||
| After watching the videos, I tried to be relaxed and avoid body tension during classes | Disagree | 3 | 37.50 | 1 | 4.00 | 4 | 12.12 | 0.036* |
| Agree | 5 | 62.50 | 24 | 96.00 | 29 | 87.88 | ||
| Before watching the videos, I was teaching in an environment that was unsuitable for teaching | ||||||||
| After watching the videos, I looked for ways to adapt the work environment to teaching | Disagree | 0 | 0.00 | 6 | 22.22 | 6 | 18.18 | 0.563 |
| Agree | 6 | 100.00 | 21 | 77.78 | 27 | 81.82 | ||
Note. Fisher's exact test. Legend: *: statistically significant value at the 5% level (p ≤ 0.05).
Table 4. Comparison of teachers according to behavior in relation to behavioral changes after the videos (cont.).
| Behavior before watching the videos | ||||||||
|---|---|---|---|---|---|---|---|---|
| Before the videos, I had little or no knowledge of voice production | ||||||||
| Behavior after watching the videos | Category | Disagree | Agree | Total | p | |||
| n | % | n | % | n | % | |||
| Before watching the videos, I was teaching classes with an inappropriate body posture | ||||||||
| After watching the videos, I started to monitor myself more and adjust my body posture during classes | Disagree | 3 | 33.33 | 1 | 4.17 | 4 | 12.00 | 0.052 |
| Agree | 6 | 66.67 | 23 | 95.83 | 29 | 87.88 | ||
| Before watching the videos, I drank less than 1.5 liters of water a day | ||||||||
| After watching the videos, I started to drink more water | Disagree | 6 | 50.00 | 0 | 0.00 | 6 | 18.18 | < 0.001* |
| Agree | 6 | 50.00 | 21 | 100 | 27 | 81.82 | ||
| Before watching the videos, I had an inadequate diet | ||||||||
| After watching the videos, I started to have a more adequate diet | Disagree | 9 | 56.25 | 1 | 5.88 | 10 | 30.30 | 0.002* |
| Agree | 7 | 43.75 | 16 | 94.12 | 23 | 69.70 | ||
| Before watching the videos, I spoke very loudly | ||||||||
| After watching the videos, I avoid speaking very loudly. | Disagree | 3 | 42.86 | 3 | 11.54 | 6 | 18.18 | 0.093 |
| Agree | 4 | 57.14 | 23 | 88.46 | 27 | 81.82 | ||
| Before watching the videos, I often shouted | ||||||||
| After watching the videos, I avoid shouting | Disagree | 6 | 54.55 | 0 | 0.00 | 6 | 18.18 | < 0.001* |
| Agree | 5 | 45.45 | 22 | 100 | 27 | 81.82 | ||
| Before watching the videos, I often cleared my throat | ||||||||
| After watching the videos, I avoid clearing my throat | Disagree | 6 | 60.00 | 2 | 8.70 | 8 | 24.24 | 0.004* |
| Agree | 4 | 40.00 | 21 | 91.30 | 25 | 75.76 | ||
| Before watching the videos, I practiced little or no physical activity | ||||||||
| After watching the videos, I started to practice more physical activity | Disagree | 8 | 53.33 | 5 | 27.78 | 13 | 39.39 | 0.169 |
| Agree | 7 | 46.67 | 13 | 72.22 | 20 | 60.61 | ||
Note. Fisher's exact test. Legend: *: statistically significant value at the 5% level (p ≤ 0.05).
Table 5. Comparison of teachers according to behavior in relation to behavioral changes after the videos (cont.).
| Behavior before watching the videos | ||||||||
|---|---|---|---|---|---|---|---|---|
| Before the videos, I had little or no knowledge of voice production | ||||||||
| Behavior after watching the videos | Category | Disagree | Agree | Total | p | |||
| n | % | n | % | n | % | |||
| Before watching the videos, I had little or no voice rest | ||||||||
| After watching the videos, I started dedicating time to resting my voice | Disagree | 4 | 40.00 | 3 | 13.04 | 7 | 21.21 | 0.161 |
| Agree | 6 | 60.00 | 20 | 86.96 | 26 | 78.79 | ||
| Before watching the videos, I paid little or no attention to my voice | ||||||||
| After watching the videos, I pay more attention to my voice and communication during class | Disagree | 4 | 33.33 | 2 | 9.52 | 6 | 18.18 | 0.159 |
| Agree | 8 | 66.67 | 19 | 90.48 | 27 | 81.82 | ||
| Before watching the videos, I used few resources other than my voice in teaching practice | ||||||||
| After watching the videos, I use more resources besides my voice in my teaching practice | Disagree | 4 | 33.33 | 4 | 19.05 | 8 | 24.24 | 0.420 |
| Agree | 8 | 66.67 | 17 | 80.95 | 25 | 75.76 | ||
| Before watching the videos, I didn't know which professional(s) to go to if I needed help with my voice | ||||||||
| After watching the videos, I know which professional(s) to go to if I need help with my voice | Disagree | 8 | 33.33 | 0 | 0.00 | 8 | 24.24 | 0.073 |
| Agree | 16 | 66.67 | 9 | 100 | 25 | 75.76 | ||
Note. Fisher's exact test. Legend: *: statistically significant value at the 5% level (p ≤ 0.05).
Perception of the teachers
The final part of the form evaluated the teachers' perception of the videos and their access feasibility and had non-mandatory open questions for teachers to comment on whether the videos lacked any information they considered important. Regarding access feasibility, teachers judged that video guidance via YouTube and email were the most accessible routes to them (66.67% of teachers chose these options), while 27.27% of participants mentioned in-person and synchronous online group guidance (by video call) as feasible for access, demonstrating that teachers consider them accessible less often. In addition, 33.33% of teachers indicated written guidance in printed materials, individual in-person guidance, and individual synchronous online guidance (by video call) as also being feasible access routes.
Twelve teachers commented on what they thought of the videos. Five of them mentioned that they lacked speech therapy exercises for vocal warm-up and cool-down, two showed an interest in health issues such as gastroesophageal reflux and hearing disorders that may directly or indirectly impact their voices, three teachers were satisfied with the videos, and one mentioned the lack of employer-centered guidance.
Finally, seven teachers added information they considered important. The main topics were the lack of vocal warm-up and cool-down exercises, difficulties in changing the work environment, and the employer's responsibility for these changes.
Discussion
This study aimed to evaluate the self-reported impact of vocal health promotion videos on teachers. Despite having been developed during the COVID-19 pandemic, the study discusses the importance of remote actions, providing easy access to appropriate information for teachers.
The study sample was well distributed in terms of age and length of teaching experience and had representatives from different Brazilian states, with a greater concentration in the state capitals. There was a predominance of females, in a similar proportion to previous studies [4,6,9].
Teachers taught predominantly in basic education (from kindergarten to high school), a finding similar to that of the population that participated in a previous study [6]. Despite the smaller sample size in the present study, the population proportionally maintained the same profile.
Evaluation of the videos
The teachers’ self-perceived effects of the videos were quite similar during different periods of the pandemic -remote classes, resuming in-person classes, and current classes- and in applying the guidelines in their daily lives. The scores were positive, demonstrating that the videos effectively provided personalized guidance according to the needs, without excluding general guidance, suitable for different work environments.
The Teacher’s Vocal Health Guide [13] was developed in 2020, gathering didactic content to be administered in collective actions in teacher vocal health. The video content evaluated in this study is in line with the instrument’s theoretical topics. However, there is a limitation to approaching practical topics such as breathing exercises, relaxation, and vocal warm-up and cool-down, as highlighted by five teachers who suggested these items be added to the videos. Nonetheless, they were intentionally not included because of the importance of having direct speech therapy guidance during the exercises to correct possible inadequacies, which would not be possible in the format chosen in the current study.
Changes after watching the videos
Most teachers mentioned changes in their vocal habits and teaching practices, but not in the work environment, and those who did described changes only in remote work, when their work environment was their home. This finding highlights the importance of including guidelines for employers to promote teachers’ vocal health and adjust the school or university environment, improving aspects such as temperature, lighting, and noise in the classroom, which influence the teachers’ health and performance [14]. In addition, it is evident that most teachers are willing to put speech therapy guidelines into practice, as observed in another study [15], but they are limited to carrying out only what is under their control, such as their habits and the strategies they use in teaching practice.
Most teachers noticed an improvement in their voices after watching the videos, but two participants noticed a worsening. This result may be related to greater vocal self-perception, identifying aspects that were not previously noticed. Another possibility is that these two teachers have some voice disorder that requires a more direct intervention, meaning the guidelines are not sufficient to modify their vocal quality. It is also possible that, despite the guidelines, they suffered a greater impact from environmental changes and mask use. Both teach children up to the 5th grade (up to 9 years old), have similar teaching experience (over 15 years), and provided below-average grades for the application of guidelines in their day-to-day life, presenting a profile similar to that observed in previous research [7]. Teachers with more in-person teaching experience suffered a greater negative impact concerning stress and vocal quality after the changes generated by the COVID-19 pandemic.
Forty-two percent of the teachers reported no change in their voices. This may have happened because the videos were not associated with a direct intervention with vocal training or individualized guidance, which would particularly benefit those who already had a vocal problem and faced vocal demands for which they were not prepared. Thus, some participants may have had difficulties perceiving improvements without vocal training.
Behaviors before and after watching the videos
Although few teachers were smokers before watching the videos, those who did tried to reduce the habit after watching them. A meta-analysis identified that smoking was related to changes in fundamental frequency and maximum phonation time and a moderate negative effect on acoustic parameters (jitter, shimmer, and noise-to-harmonic ratio) and the Voice Handicap Index - VHI [16]. Another study [17] found no association between smoking and voice disorders in teachers, but the author points out that this result could be related to the small sample, requiring new longitudinal studies. Therefore, it is inferred that reduced smoking, which is an essential guideline in this type of action, positively impacts teachers’ voices and prevents possible voice disorders.
Teachers who consumed alcohol were less inclined to reduce their consumption after watching the videos. This finding may related to their being a social/sporadic habit, so that there was no perceived need to reduce it. However, attention must be paid to this aspect because depending on the dose and frequency of consumption, alcohol is related to acute and chronic voice disorders [18].
Teachers sought to increase water consumption after viewing the videos. It is interesting to note that mask use as they resumed in-person classes led teachers to decrease their daily water intake and increase vocal complaints [19]. Therefore, the videos not only raised awareness about the importance of water intake for the voice, but also helped teachers overcome the tendency to reduce their consumption as in-person classes resumed.
The habits of shouting and clearing the throat also changed after watching the videos. This result is extremely relevant since, as evidenced in a previous study [20], the perception of voice improvement during the COVID-19 pandemic was directly related to reducing the habits of shouting and clearing the throat, whereas these vocal abuse habits were directly related to the perception of worsened vocal quality.
After watching the videos, teachers tried to be more relaxed and avoid body tension during classes. A systematic review [21] showed a relationship between posture, muscle tension, and voice, as even subtle postural changes in the head, spine, or balance can influence muscle stability and reduce the efficiency of laryngeal movement, leading to greater vocal strain and changes in voice quality, pitch, and resonance. In addition, teachers tend to maintain greater rigidity and postural tension, which may result in -or from- dysphonia, as more muscle compensation is performed to achieve a desired vocal pattern. Thus, paying attention to postural aspects can reduce these teachers’ vocal effort and improve their communication.
Finally, the participants tried to improve their eating habits after viewing the videos. A study [22] identified that most teachers had unhealthy eating habits (diets low in fruits and vegetables and high in fast food, with undefined meal schedules) and reported a stressful routine, lack of time, and anxiety, which affected their daily food choices. These habits can lead to changes in body weight and volume, influencing their fundamental frequency and maximum phonation time [23] and predisposing them to diseases such as gastroesophageal reflux that directly or indirectly influence voice and communication [24]. Thus, seeking to improve eating habits positively impacts general and vocal health [25].
Perception of the teachers
Most teachers demonstrated that remote actions are more viable for access. As shown in previous studies [18,19], such actions with easily accessible online materials effectively help them learn the concepts addressed, as teachers can resume the content whenever necessary, with greater flexibility of access times, and without needing to travel to a specific location for in-person attendance. Due to the extensive workload and work organization often reported as stressful [21], teachers need health actions adapted to their reality, aiming at greater adherence and impact. It is also important to consider aspects of mental health, general health, and the work environment for the development of speech therapy actions for teachers.
Limitations and recommendations
The present study has limitations. The small sample size and the concentration of the sample in more socioeconomically favored regions reduce the statistical power of the analyses and hinder their generalization. In addition, some questions or evaluations in the questionnaire depended on the participants’ interpretation and memory, which can generate biased results.
Nonetheless, the study confirmed its initial hypothesis, demonstrating that the research contributes to the literature focused on teachers’ vocal health and differs from previous research by addressing this topic from the perspective of changes generated at different health moments during the COVID-19 pandemic. For future research, it would be interesting to carry out a longitudinal study with the same population to understand whether they maintained their habits and behavioral changes. Moreover, a third video addressing the topics suggested by the teachers could complement the action.
Conclusions
The videos stimulated self-perception and facilitated changes, positively impacting the teachers’ voices and communication. The participants evaluated the videos positively and reported changes in their vocal habits and teaching practices. They also noticed improvements in their voices after watching the videos. The modified behaviors included reduced smoking, increased water intake, reduced habit of shouting and clearing their throat, being more relaxed and without tension during classes, and improved eating habits. Finally, most teachers mentioned that remote speech therapy guidance with online materials is the most viable access route, emphasizing that more actions of this type should be developed, using these videos to promote vocal health and disseminating them so that teachers can review the guidelines whenever necessary.
References
1. Behlau M, Zambon F, Guerrieri AC, Roy N. Epidemiology of voice disorders in teachers and nonteachers in Brazil: prevalence and adverse effects. J Voice [Internet]. 2012;26(5):665.e9-665.e18. doi: https://doi.org/10.1016/j.jvoice.2011.09.010
2. Van Houtte E, Claeys S, Wuyts F, Van Lierde K. The impact of voice disorders among teachers: vocal complaints, treatment-seeking behavior, knowledge of vocal care, and voice-related absenteeism. J Voice [Internet]. 2011;25(5):570-5. doi: https://doi.org/10.1016/j.jvoice.2010.04.008
3. Medeiros AM de, Vieira MT. Work absenteeism due to voice disorders in Brazilian school teachers. Cad Saúde Pública [Internet]. 2019;35(Suppl1):e00171717. doi: https://doi.org/10.1590/0102-311X00171717
4. Lu D, Wen B, Yang H, Chen F, Liu J, Xu Y, et al. A comparative study of the VHI-10 and the V-RQOL for quality of life among Chinese teachers with and without voice disorders. J Voice [Internet]. 2017;31(4):509.e1-509.e6. doi: https://doi.org/10.1016/j.jvoice.2016.10.025
5. Lyberg-Åhlander V, Brännström KJ, Sahlén BS. On the interaction of speakers' voice quality, ambient noise and task complexity with children's listening comprehension and cognition. Front Psychol [Internet]. 2015;6:1-5. doi: https://doi.org/10.3389/fpsyg.2015.00871
6. Nemr K, Simões-Zenari M, Almeida VC de, Martins GA, Saito IT. COVID-19 and the teacher’s voice: self-perception and contributions of speech therapy to voice and communication during the pandemic. Clinics [Internet]. 2021;76:e2641. doi: https://doi.org/10.6061/clinics/2021/e2641
7. Cantor-Cutiva LC. Relationship Between Room Acoustics with Voice Symptoms and Voice-Related Quality of Life Among Colombian School and College Teachers During Online Classes in Times of COVID-19 Pandemic. J Voice [Internet]. Forthcoming 2022 Mar 13. doi: https://doi.org/10.1016/j.jvoice.2022.03.008
8. Besser A, Lotem S, Zeigler-Hill V. Psychological Stress and Vocal Symptoms Among University Professors in Israel: Implications of the Shift to Online Synchronous Teaching During the COVID-19 Pandemic. J Voice [Internet]. 2022;36(2):291.e9-291.e16. doi: https://doi.org/10.1016/j.jvoice.2020.05.028
9. Pizolato RA, Rehder MIB, Meneghim M de C, Ambrosano GMB, Mialhe FL, Pereira AC. Impact on quality of life in teachers after educational actions for prevention of voice disorders: a longitudinal study. Health Qual Life Outcomes [Internet]. 2013;11:28. doi: https://doi.org/10.1186/1477-7525-11-28
10. Nallamuthu A, Boominathan P, Arunachalam R, Mariswamy P. Outcomes of Vocal Hygiene Program in Facilitating Vocal Health in Female School Teachers with Voice Problems. J Voice [Internet]. 2023;37(2):295.e11-295.e22. doi: https://doi.org/10.1016/j.jvoice.2020.12.041
11. Grillo EU. A Nonrandomized Trial for Student Teachers of an In-Person and Telepractice Global Voice Prevention and Therapy Model with Estill Voice Training Assessed by the VoiceEvalU8 App. Am J Speech Lang Pathol [Internet]. 2021;30(2):566-83. doi: https://doi.org/10.1044/2020_AJSLP-20-00200
12. Penha PB da C, Lima Filho LM de A, Ferreira LP, de Almeida AAF, Lopes LW, Silva MF de L. Effectiveness of a Blended-Learning Intervention in Teachers' Vocal Health. J Voice [Internet]. 2023;37(4):635.e1-635.e13. doi: https://doi.org/10.1016/j.jvoice.2021.03.012
13. Aoki MC de S, Santos RS, Brasolotto AG. Presentation and evaluation of the Teacher's Vocal Health Guide. J Voice [Internet]. 2022;36(4):531-7. doi: https://doi.org/10.1016/j.jvoice.2020.07.009
14. Marçal CCB, Heidemann ITSB, Durand MK, Rumor PCF, Arakawa-Belaunde AM, de Souza JM. Salutogenic resources for promoting teachers’ vocal health. Rev CEFAC [Internet]. 2021;23(3):1-10. doi: https://doi.org/10.1590/1982-0216/202123310320
15. Porcaro CK, Howery S, Suhandron A, Gollery T. Impact of Vocal Hygiene Training on Teachers' Willingness to Change Vocal Behaviors. J Voice [Internet]. 2021;35(3):499.e1-499.e11. doi: https://doi.org/10.1016/j.jvoice.2019.11.011
16. Byeon H, Cha S. Evaluating the effects of smoking on the voice and subjective voice problems using a meta-analysis approach. Sci Rep [Internet]. 2020;10(1):4720. doi: https://doi.org/10.1038/s41598-020-61565-3
17. Byeon H. The Risk Factors Related to Voice Disorder in Teachers: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health [Internet]. 2019;16(19):1-14. doi: https://doi.org/10.3390/ijerph16193675
18. Rossi-Barbosa LAR, Barbosa MR, Morais RM, de Sousa KF, Silveira MF, Gama ACC, et al. Self-Reported Acute and Chronic Voice Disorders in Teachers. J Voice [Internet]. 2016;30(6):755.e25-755.e33. doi: https://doi.org/10.1016/j.jvoice.2015.08.003
19. Furnas DW, Wingate JM. The Effects of Mask Usage on Reported Vocal Health of Educators. J Voice [Internet]. Forthcoming 2022 May 31. doi: https://doi.org/10.1016/j.jvoice.2022.04.011
20. Nemr K, Simões-Zenari M, Cologis VCA, Martins GA, Saito IT, Gonçalves RS. COVID-19 and Remote Learning: Predictive Factors of Perceived Improvement or Worsening of the Voice in Brazilian Teachers. J Voice [Internet]. 2024;38(1):246.e27-246.e38. doi: https://doi.org/10.1016%2Fj.jvoice.2021.08.010
21. Cardoso R, Lumini-Oliveira J, Meneses RF. Associations between Posture, Voice, and Dysphonia: A Systematic Review. J Voice [Internet]. 2019;33(1);124.e1-124.e12. doi: https://doi.org/10.1016/j.jvoice.2017.08.030
22. Vio F, Yañez M, González CG, Fretes G, Salinas J. Teachers’ self-perception of their dietary behavior and needs to teach healthy eating habits in the school. J Health Psychol [Internet]. 2018;23(8):1019-27. doi: https://doi.org/10.1177/1359105316642003
23. Souza LBR, Santos MMD. Body mass index and acoustic voice parameters: is there a relationship? Braz J Otorhinolaryngol [Internet]. 2018;84(4):410-5. doi: https://doi.org/10.1016/j.bjorl.2017.04.003
24. Ricci G, Wolf AE, Barbosa AP, Moreti F, Gielow I, Behlau M. Signs and symptoms of laryngopharyngeal reflux and its relation to complaints and vocal quality. CoDAS [Internet]. 2020;32(5):1-5. doi: https://doi.org/10.1590/2317-1782/20202018052
25. Fontes VS, de Oliveira CG. Food as a relevant factor to vocal health: foods that provide benefits and harm effects to vocal production. HU Rev [Internet]. 2016;42(1):19-25. Available from: https://periodicos.ufjf.br/index.php/hurevista/article/view/2328