
Family Functioning as a Possible Factor that Modulates Empathy Levels in Dental Students
Funcionamiento Familiar como posible factor que modula los niveles de empatía en estudiantes de odontología
Nuvia Estrada-Méndez, Jennifer Elizabeth Aldana Salguero, Brenda Nathaly Alfaro Ortiz, Aracelis Calzadilla-Núñez, Alejandro Reyes-Reyes, Víctor Patricio Díaz-Narváez
Abstract
Aim: The objective of this paper is to explore whether there are differences in the levels of empathy and its dimensions between family typologies in dental students.
Methodology: A quantitative and not experimental study, with a cross-sectional descriptive design, a population of dental students from the Evangelical University of El Salvador, and a convenience sample were applied. The levels of empathy and family functioning were evaluated using the Jefferson Scale of Empathy for Health Professions students and the Brief Scale of Family Functioning. The construct validity of both instruments was estimated using Confirmatory Factor Analysis. The reliability was estimated using McDonald's omega and Cronbach's alpha. Comparisons of empathy and its dimensions between family typologies were made using a two-factor analysis of variance.
Results: No statistical differences were observed in empathy and its dimensions based on family typologies. It was found that women are more empathic than men. This result is not in accordance with other studies carried out in Latin America on dental and medical students evaluating empathy and family functioning with the same instruments.
Conclusions: The distribution of empathy levels and their dimensions are similar among the family typologies studied. Therefore, it was not found that family functioning can influence empathy in the population studied. It is necessary to continue these studies to obtain more empirical evidence regarding the influence of family functioning on empathy.
Keywords
Empathy; family; students; dentistry; reliability; family functioning; psychological resilience.
Resumen
Objetivo: El objetivo del presente trabajo es determinar la existencia de diferencias de los niveles de empatía y de sus dimensiones entre las tipologías familiares en estudiantes de odontología.
Metodología: Estudio cuantitativo y no experimental, con un diseño descriptivo transversal, una población de estudiantes de odontología de la Universidad Evangélica de El Salvador y una muestra por conveniencia. Fueron evaluados los niveles de empatía y el funcionamiento familiar mediante la Escala de Empatía de Jefferson para estudiantes de profesiones de la salud y la Escala Breve de Funcionamiento Familiar. Se estimó la validez de constructo de ambos instrumentos mediante Análisis Factorial Confirmatorio y la confiabilidad mediante omega de McDonald y alfa de Cronbach. Las comparaciones de la empatía y sus dimensiones entre las tipologías familiares fueron realizadas mediante análisis de varianza bifactorial.
Resultados: No se observaron diferencias estadísticas en la empatía y en sus dimensiones en función de las tipologías familiares. Se encontró que las mujeres son más empáticas que los hombres. Este resultado no está en concordancia con otros estudios realizados en América Latina en estudiantes de odontología y medicina, evaluando la empatía y el funcionamiento familiar con los mismos instrumentos.
Conclusiones: La distribución de los niveles de empatía y de sus dimensiones son semejantes entre las tipologías familiares estudiadas. Por lo tanto, no se constató que el funcionamiento familiar tenga un efecto sobre la empatía en la población estudiada. Es necesario continuar estos estudios para obtener mayor evidencia empírica respecto de la influencia del funcionamiento familiar en la empatía.
Palabras clave
Empatía; familia; estudiantes; odontología; confiabilidad; funcionamiento familiar; resiliencia psicológica.
Introduction
Medical empathy is an attribute that allows the intersubjective relationship between the patient and the treating dentist [1] and contributes to better adherence to treatment, a decrease in patient stress and complaints about the care received, among other aspects that have been described by several different authors [1-4]. Medical empathy has two components: cognitive and emotional. Some authors have pointed out that empathy is fundamentally cognitive, while others argue that empathy is a system where these two components have a dialectical relationship between them and cannot be separated at the time of caring for a patient [2-4]. The Jefferson Empathy Scale is an instrument that measures the levels of Empathy (E) in professionals and students of health sciences and is constituted by three dimensions (subscales): Compassionate Care (CC), Perspective Taking (PT) and “Walking in the Patient's Shoes” (WPS). The first one is associated with the emotional sphere of the patient, while the others are associated with the cognitive sphere [1-4]. These three structures determine the correct prosocial behavior when they work in coordination [5]. These three dimensions are supported by independent neurological structures; however, they are connected by neural networks that allow their interaction [6-8]. The emotional component is associated with the limbic system while the cognitive one is associated with the frontal orbit part of the brain [6-9].
The development of empathy is under pressure from phylogenetic and ontogenetic factors perspective [9,10]. Currently, the factors specifically associated with ontogeny are the ones that mostly influence the positive or negative consolidation of this attribute in a human being [10]. Therefore, the study of empathic behavior must involve knowledge of the factors that can positively or negatively influence its development. Such knowledge could contribute to a correct interpretation of the observed results of empathy levels in a given population. Empathic erosion is an example of how various factors such as stress, excessive academic workload, and the bad example of the teacher, among others, have the effect of destabilizing the functioning of empathy with the patient and manifests itself with an increase in the compassionate threshold and a deterioration in the ability to understand what the patient is thinking and feeling. The consequence of this empathic erosion is a decrease in empathy levels. The literature argues that this phenomenon of empathic decline usually occurs when the student begins his academic activity in the clinical area [1-4,10].
The family is a constant element in a person's life and holds significant importance during the time span from birth to early adulthood. [11-13]. Therefore, this can be a "suspected" factor in modulating a person's empathic behavior. The family ceases to be an abstract concept provided one can establish typologies that allow observing whether empathic behavior is distributed differently among such typologies. In this sense, the FACES III (Family Adaptability and Cohesion Evaluation Scale) instrument (Faces-20-Esp) [14-16] is one of the instruments used to assess family functioning [17]. It is based on Olson's circumplex model of family and marital systems [14,16]. This instrument allows for distinguishing between balanced, intermediate-range, and extreme families, thus transitioning from functional to dysfunctional ones.
Therefore, the study of the possible modulation of Family Functioning on empathy is important to understand if such functioning can predict empathic behavior, assuming that this influence cannot necessarily be observed, since empathy is influenced by many factors at the same time [1-5]. The objective of this study is to determine whether there are differences in the levels of empathy and its dimensions among family typologies in dental students.
Methodology
Type of study and design
This was a quantitative, non-experimental study with a descriptive and cross-sectional design [18].
Variables
Dependent: Empathy. Dimensions of empathy: Compassionate Care (CC) (8 items), Perspective Taking (PT) (10 Items), and “Walking in the Patient's Shoes” (WPS) (2 Items). Independent: Family Functioning. Fixed factors: Typologies of Family Functioning (FT) and Sex(S). Covariate: Course (C).
Participants
The population consists of all dentistry students at Universidad Evangelica de El Salvador evaluated in 2022 (N = 462; Women = 329; Men = 133).
Sample
The sample was comprised of 397 students of both sexes, selected in a non-probabilistic way for convenience [18] and it was obtained from all the students who voluntarily agreed to respond to the two applied instruments (JSE-HPS version and Faces-20-Esp.), after signing the informed consent
Inclusion criteria
Every student who agreed to respond to the instrument voluntarily, everyone who had a regular-student status (from the basic, preclinical, or clinical area) who were present at the time of the instrument application.
Exclusion criterion
Turning in incomplete instruments.
Data collection strategy
The data were collected by professors of the School of Dentistry. The informed consent and the instruments that measure empathy and discriminate family typologies were applied in paper format and in person during class time. Professors had been trained for the correct application and reception of the answers. The data were tabulated in Excel tables for further processing.
Instruments
Empathy
The empathy measurement was performed using the Jefferson Empathy Scale (JSE) version for students of health professions (HPS-Version) [18-20]. This instrument has 20 items in Likert scale format, with response levels from 1 to 7, and has been well described by several authors [1-4]. Operationalization: The empathy variable can be measured by quantifying the score that can fluctuate between 20 and 140 points, that is, CC (56 points), PT (70 points), and WPS (14 points).
Family Functioning
The Brief Family Functioning Scale, Spanish version (Faces-20-Esp), has been validated in Spain [19] and Chile [20]; it has 20 items in Likert scale format, graded from 0 to 4 points, which presents statements about situations that occur in family life. The value 0 = “Never”, 1 = “Almost never”, 2 = “Rarely”, 3 = “Frequently” and 4 = “Almost always”. It measures two dimensions: Cohesion (items 1, 4, 5, 8, 10, 11, 13, 15, 17, and 19) and Adaptability (items 2, 3, 6, 7, 9, 12, 14, 16, 18 and 20). The dimension of Cohesion can be subdivided into four levels: Disengaged · Separated · Connected · Enmeshed. The Adaptability dimension is also made up of four levels: Rigid, Structured, Flexible, and Chaotic. From the combinations of the levels of cohesion and adaptability, the family typology can be extracted: Balanced, Intermediate and Extreme: the Extreme indicates a family malfunction and the Balanced denotes good family functioning [20]. Operalization: The variable can be measured by quantifying the score that can fluctuate between 0 and 80 points.
Judges' criteria
Before the application of both instruments, it was submitted to judges' criteria (dental surgeons, psychologists, educators, and higher education experts) to obtain evidence of content validity.
Pilot test
Both instruments were applied to 30 students including all courses and both sexes [2].
Statistical analysis
Psychometric Properties
Both instruments were statistically examined by the same procedures. For the Confirmatory Factor Analysis (CFA) the Robust Maximum Likelihood estimator (MLR) was used [21], which is characterized by being robust in the absence of multivariate normality of the data. [22] The RMSEA, SRMR, CFI and TLI indices were used to evaluate the fit of the models. Values less than 0.08 were considered acceptable for the RMSEA and SRMR indices, [23]. Values greater than 0.90 were considered acceptable for the CFI and TLI indices, [24]. The evaluation of the reliability of the scale was estimated by Cronbach's alpha coefficient (α) and omega coefficient (ω), where a value ω>0.80 is suitable [25].
The Multi-group Confirmatory Factor Analysis (MGCFA) was used to measure the factor invariance of the scale according to sex, in which a sequence of four hierarchical variance models was proposed: configural invariance (reference model), metric invariance (equality of factor loads), scalar invariance (equality of factor load and intercept) and strict invariance (equality of factor loads, intercept and residuals). A modeling strategy was used to compare the sequence of models, for which the differences in the RMSEA (ΔRMSEA) were used, where differences less than <0.015 evidence the invariance of the model between the groups [24]. The differences in the CFI (ΔCFI) were also used, in which values less than <0.010 show the invariance of the model between the groups [26,27]. The univariate and multivariate normality of the data was analyzed, providing the kurtosis and asymmetry and Mardia test, respectively [28]. The psychometric study was carried out to confirm that the data observed in the present study comply with the FF and Empathy models and their respective underlying dimensions.
Comparison of empathy levels between family typologies
The mean and the standard deviation of the empathy levels (and their dimensions) were calculated in each of the two studied factors: Family Typology (FT) and Sex (S). The Course factor (C) was considered a covariate. The primary data of empathy observed in each of the FT were compared by means of a bifactorial analysis of variance (ANOVA), in order to measure the presence of differences between the FT and between the sexes. The interaction between the FT and S factors (FT*S) was calculated. The effect size was calculated (ἠ2=eta squared) to determine whether the differences between the variables of the compared samples were large or small, [29] and the test power (PT) was calculated to determine the magnitude of the type II error (1-β) [30]. The application of all these methods allows reliable comparisons to be made.
Mplus 8 was used for the confirmatory factor analysis and the invariance analysis, [31], making use of SPSS 29 (IBM Corp., 2020) for the other analyses. The significance level used in all cases was α<0.05 and β>0.80.
Ethical aspects
The study was conducted under the ethical principles of the Declaration of Helsinki (2013). The research project, as well as the informed consent, were approved by the Ethics Committee of the Evangelical University of El Salvador (UEES): Act N° 307/08/2022. All sociodemographic, personal data and the responses of the instrument applied, as well as the informed consent, are confidential.
Results
The sample consisted of 397 (n) students, out of a total of 462 (N) (85.93% of the studied population), between the first and seventh course. Distributed in 293 female students (73.8%) and 104 (26.2%) male. With a mean age of 21.49 years (SD=2.79).
Compliance with the model
It was evidenced that the original empathy model of three related factors presents adequate adjustment indices (χ2 = 329.87; gl = 167; p <. 01; CFI =. 92; TLI =.91; RMSEA =. 056 [90% CI,047 ‒ .064]; SRMR = .057). Factorial Invariance: It was found that the factorial structure of the scale has shown evidence of being strictly invariant for the groups of men and women in the sequence of proposed invariance models: metric invariance (ΔCFI = -0.001; ΔRMSEA = -0.002), scalar (ΔCFI = -0.010; ΔRMSEA = 0.002) and strict (ΔCFI = -0.003; ΔRMSEA = -0.001).
The dimensions of the empathy scale present adequate reliability indices: Perspective Taking or Perspective Adoption (α=0.89; ω=0.89), Compassionate care (α=0.79; ω=0.79), and Putting oneself in the patient's shoes (α=0.68; ω=0.71). Similarly, in the sample of women, all three dimensions presented acceptable reliability indices: Perspective Taking (α=0.89; ω=0.89), Compassionate Care (α=0.77; ω=0.78) and Putting oneself in the Patient's Shoes (α=0.64; ω=0.65). In the sample of males, the three dimensions also presented adequate adjustment indices: Adoption of Perspective (α=0.89; ω=0.90), Compassionate Care (α=0.83; ω=0.84), and Putting oneself in the Patient's Shoes (α=0.74; ω=0.76).
In the case of the family functioning variable, it is appreciated that the vast majority of the items present adequate asymmetry and kurtosis indices (As < ±2; Kurt < ±7) according to the criteria of Finney and DiStefano [32], but lacking multivariate normality with a multivariate kurtosis of 111.08. Factorial validity: A two-factor model correlated with a good result of the goodness of fit test was finally obtained (χ2 = 284.06; gl = 163; p < 0.0001; RMSEA = 0.071 [90% CI 0.057-0.084.]; (IFC=0.89; TLI=0.87; SRMR=0.057). This model presents high and significant standardized factor loads (λ), which in general are greater than 0.50. Reliability: The dimensions of the family functioning scale have adequate reliability indices: α (Cohesion)=0.89, α (Adaptability)=0.88, observing the reliability of the measure, by using McDonald's omega coefficient of ω=0.96.
Estimation of statistics and comparison of empathy levels in family typologies
In Table 1 the results of the distribution of the means and standard deviations of empathy and their dimensions as a function of FT and S are presented. From the perspective of the absolute values, it was observed that women have, in general, higher E, CC, TP, and CZP values than men (see Figure 1). In Table 2, it was observed that the E and none of its dimensions differ statistically between the FT, but in the S factor, where women have higher values of E, CC, and CZP; there were no differences in the TP dimension. The present study shows that in the studied population the absence of statistical significance of the Course covariate does not affect the distribution of the dependent variable as a function of FT and S. However, it is necessary to emphasize that the value of the effect size and the power of the test were not satisfactory; such value shows that the statistical differences found are small.
Table 1. Distribution of the means of empathy and its dimensions among the examined family typologies
| Family Typology | Sex | Mean E | Standard Deviation E | Mean CC | Standard Deviation | Mean PT | Standard Deviation PT | Media WPS | Standard Deviation WPS | n |
|---|---|---|---|---|---|---|---|---|---|---|
| Extreme | Male | 95.91 | 17.891 | 30.94 | 12.331 | 58.57 | 9.960 | 6.40 | 3.041 | 35 |
| Female | 100.17 | 16.688 | 35.67 | 9.947 | 56.69 | 11.713 | 7.81 | 2.879 | 120 | |
| Total | 99.21 | 17.001 | 34.60 | 10.675 | 57.12 | 11.337 | 7.49 | 2.966 | 155 | |
| Balanced | Male | 94.77 | 14.718 | 32.94 | 9.568 | 55.15 | 9.695 | 6.68 | 2.883 | 47 |
| Female | 99.35 | 16.020 | 35.07 | 9.537 | 57.38 | 9.481 | 6.91 | 2.391 | 88 | |
| Total | 97.76 | 15.678 | 34.33 | 9.567 | 56.60 | 9.579 | 6.83 | 2.564 | 135 | |
| Intermediate | Male | 94.27 | 16.063 | 32.27 | 10.138 | 55.18 | 8.937 | 6.82 | 2.684 | 22 |
| Female | 99.62 | 15.249 | 34.48 | 10.033 | 57.54 | 9.665 | 7.60 | 2.629 | 85 | |
| Total | 98.52 | 15.496 | 34.03 | 10.047 | 57.06 | 9.527 | 7.44 | 2.646 | 107 | |
| Total | Male | 95.05 | 15.982 | 32.13 | 10.621 | 56.31 | 9.676 | 6.62 | 2.874 | 104 |
| Female | 99.76 | 16.030 | 35.14 | 9.830 | 57.14 | 10.474 | 7.48 | 2.686 | 293 | |
| Total | 98.53 | 16.132 | 34.35 | 10.117 | 56.92 | 10.266 | 7.25 | 2.759 | 397 |
Note.E: Empathy. CC: Compassionate Care. PT: Perspective Taking; WPS: "Walking in the Patient's Shoes."
Figure 1. Value of empathy means and each of its dimensions in Family Typologies
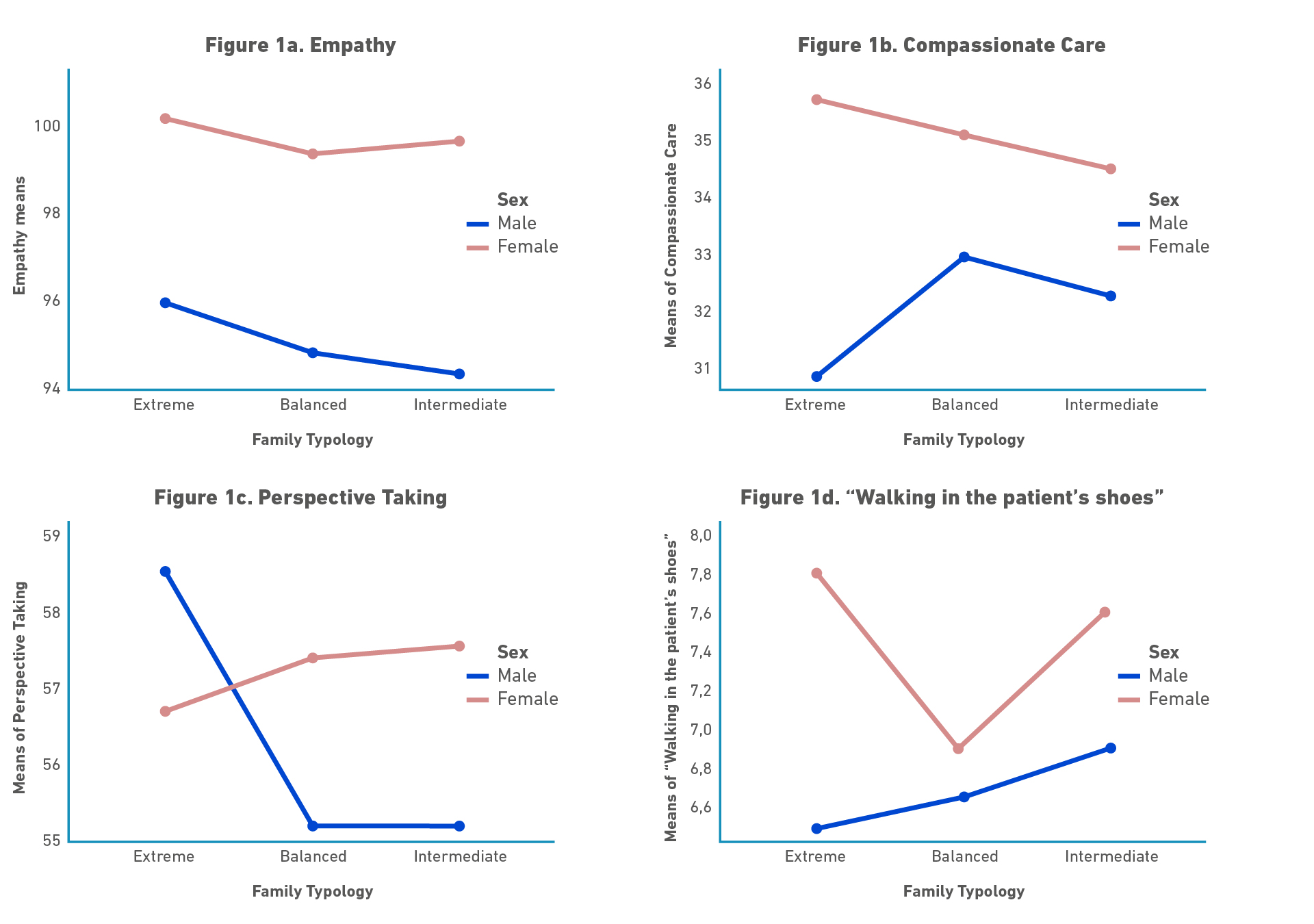
Table 2. Results of the analysis of factor variance in Empathy and in each of its dimensions.
| Empathy and its dimensions | F | Statistical significance | Partial Eta squared (ἠ2) | Observed power (PT) |
|---|---|---|---|---|
| Empathy | ||||
| Course | 0.003 | 0.955 | 0.0005 | 0.050 |
| FT | 0.142 | 0.868 | 0.001 | 0.072 |
| Sex | 6.057 | 0.014 | 0.015 | 0.690 |
| FT * Sex | 0.025 | 0.975 | 0.0005 | 0.054 |
| Compassionate Care | ||||
| Course | 0.029 | 0.866 | 0.0005 | 0.053 |
| FT | 0.170 | 0.844 | 0.001 | 0.076 |
| Sex | 6.400 | 0.012 | 0.016 | 0.713 |
| FT * Sex | 0.569 | 0.566 | 0.003 | 0.144 |
| Perspective Taking | ||||
| Course | 0.044 | 0.834 | 0.0005 | 0.055 |
| FT | 0.557 | 0.573 | 0.003 | 0.142 |
| Sex | 0.566 | 0.452 | 0.001 | 0.117 |
| FT * Sex | 1.384 | 0.252 | 0.007 | 0.297 |
| "Walking in the patient's shoes” | ||||
| Course | 3.089 | 0.080 | 0.008 | 0.418 |
| FT | 0.849 | 0.429 | 0.004 | 0.196 |
| Sex | 5.521 | 0.019 | 0.014 | 0.649 |
| FT * Sex | 1.138 | 0.322 | 0.006 | 0.250 |
Note. FT: Family Typology; *: Interaction between the factors studied.
Family functioning is important because it actively instills moral values, elicits affection, builds emotions, and teaches prosocial behaviors [1-5] among many more virtues[1-4]. Well-constituted moral values and positive affections are predictors of high levels of empathy [2,3].
The fact that, in the present work, there were no differences in the levels of empathy and its dimensions between family typologies does not imply that this situation is the same in other student populations. In other words, theoretically speaking, family functioning can be "negative”, but the general context where the person develops can be positive and empathy may not be affected by a family malfunction. The results observed in this work, therefore, could constitute an important empirical element that could help to hypothetically understand that family functioning acts on empathy within an ontogenic context. In turn, it can inform us indirectly that empathy is modulated by the presence of other factors that also participate in such modulation that act simultaneously with family functioning. However, the scarce existing empirical information limits the possibility of theorizing about it and shows the need to continue researching how empathy levels are distributed depending on family typology in a massive way to accumulate the critical empirical evidence necessary to generate well-founded hypotheses.
Discussion
The observed results allow us to infer that the three-dimensional model of empathy and two-dimensional family functioning are fulfilled in the studied sample. Additionally, the results of the fulfillment of invariance between groups (sex) are also fulfilled. These results validate the comparisons of the distribution of empathy and its dimensions; and the comparisons between male and female sex according to family typology. The sample studied was not representative of the population. However, this problem cannot be solved, since the population is naturally finite, so it cannot be artificially increased. Furthermore, in the context of voluntary participation, 100% of the population cannot be evaluated.
In relation to empathy and its dimensions, the studies carried out in Latin America let us observe some characteristics that seem to be typical of this continent. First of all, it was proved, in dentistry students, that there is variability in the distribution of the means of empathy between the courses and sex [2,33-36]. The same situation occurs with other specialties of health sciences [37,38]. In fact, it has been observed that there are six different forms of empathy behavior between courses in dental students; in addition, empathy between the sexes does not always favor females. In some cases, no differences have been found between the two sexes, in others, the male students have demonstrated higher levels of empathy than women. These observations contradict the concept of declination that has been assumed as a constant [1-4]. Such a concept has also been described as the sharp decrease in empathy from the moment students in dentistry, medicine, and other health specialties [1-4,6-13].
There are authors who have suggested that a possible explanation for this variability is that empathy is an attribute that is slowly being built up along the processes associated with ontogeny [2,3,10]. Indeed, some factors such as stress, excessive evaluations, the negative behavior of the teacher towards students, the way he treats patients, the academic climate, and resilience, among other factors, are related to "empathic erosion”, which potentially tend to modify the levels of empathy since entering to the preclinical or clinical areas [33-38]. However, it has been observed in some dental schools that the average levels of empathy have increased, despite the factors described above, being present, at least to some extent [35,36].
If empathy seems to be the result of the action of several factors that modulate empathic training from the point of view of its architecture, as well as its functioning [1-13], then family functioning could be an important component to explain, at least in part, empathic behavior.
In the case of family functioning, there are very few studies that analyze the psychometry of this instrument, but in all of them, it has been observed that this construct has two dimensions (Cohesion and Adaptability), confirming the results of the present work [20,39-41]. On the other hand, there are also few studies that have tried to link empathy with family functioning through the use of Faces-20-Esp [42,43]. In this regard, the cited works it was found that the type of extreme family functioning has higher empathy values in relation to the other typologies of family functioning and concluded that this family typology could contribute to some aspects associated with the formation of empathic values. An attempt to interpret this result could be that authoritarian or absent leadership, which characterizes the qualification of "extreme typology," affects communication [44]. But this relationship has been criticized mainly for the simplistic form of characterization that exists in family communication or simply for considering extreme typology as erratic [17,43]. On one hand, it could be considered that this typology is influenced by culture; therefore, the development of the subject under certain cultures would not affect communication in the context of extreme families [42-45]. On the other hand, we could assume that dental students are people with a high IQ. Therefore, although they were raised in a family of extreme characteristics, they could have developed resilience and somehow they “cancel out” the negative effect that the condition of extreme family functioning would have on empathy [46-49]. To summarize, trying to explain how the family and, specifically, family functioning influences empathy is a complex task and it is beyond the scope of this work.
In fact, if the considerations made above are plausible, it could be inferred that the modulation of family functioning on empathy is variable, and empathy would be the result of a particular complex correlation of the different factors that contribute to the modulation of this attribute in each of the populations studied. This situation could explain the variability (different results) observed so far, in relation to the distribution of empathy levels according to family typologies. The reason seems to be “simple": not all factors influence empathy equally in different populations. However, this inference, to be admitted as a scientific fact, requires more empirical evidence. The one existing so far is not sufficient to theorize about it. In this context, the empirical evidence obtained in this work would be a manifestation of the variability described above and, as a consequence, could lead us to consolidate a consistent tendency to describe that family functioning can effectively modulate empathy, which supports the hypothesis of some authors [42-43] that consider empathy as a result of the influence of many factors acting at the same time and that such influence necessarily determines variable results.
As a consequence, there is a need to determine, in all possible contexts, [50] how empathy levels are distributed according to family typologies. As a consequence, it is likely that we are in the presence of a problematic system rather than just a simple problem, [18,51], which is, of course, more complex to solve than the determination described above.
Conclusions
The neutrality in the distribution of empathy levels in the family typologies found may be a manifestation of the presence of variability in the distribution of empathy (and its dimensions) in relation to family functioning. These studies should be complemented with those which will allow us to know the possible motivations and thoughts that determined students' responses to the instruments.
Limitations and recommendations
The main limitation is that the conclusions obtained are local in nature and the study of the relationship between empathy and family functioning has been scarcely studied. It is recommended to evaluate other populations of dental students, as well as other specialties, with the aim of accumulating empirical evidence regarding the way in which empathy levels are distributed and their dimensions based on the classifications of family typologies.
References
1. Moore R. Maximizing Student Clinical Communication Skills in Dental Education-A Narrative Review. Dent J (Basel). 2022;10(4):57. doi: https://doi.org/10.3390/dj10040057
2. Fortich Mesa N, Díaz-Narváez VP. Actitud empática en estudiantes de odontología de la Corporación Universitaria Rafael Núñez en la ciudad de Cartagena. Rev. Cienc. de la Salud. 2018;16(1):129-143. doi: https://doi.org/10.12804/revistas.urosario.edu.co/revsalud/a.6495
3. Torres-Martínez PA, Barrios-Penna CA, Fonseca-Molina JF, Díaz- Narváez VP, González-Cruz SA. Levels of empathy in dental students at Universidad San Sebastián in Concepción, Chile. Rev. Fac. Med. 2017;65(2):219-25. doi: https://dx.doi.org/10.15446/revfacmed.v65n2.61444
4. Díaz-Narváez VP, Calzadilla-Núñez A. Ecualización de la empatía en estudiantes de dos sedes diferentes en una facultad de odontología de una universidad chilena. Rev Med Rosario. 2019;85(1):020-026. Disponible en: https://revistamedicaderosario.org/index.php/rm/article/view/17
5. López Arboleda GM, Betancur Vélez A, Bustamante Rodríguez A, Uribe Figueroa AM, Ortiz González AL, Agudelo Zorrilla AF, et al. Amor, empatía y conductas prosociales: una reflexión interdisciplinaria. Gloria María López Arboleda, Diego Alejandro Pérez Múnera, Editores. Medellín: Fondo Editorial Universidad Católica Luis Amigó; 2022. p. 225. Disponible en: https://tinyurl.com/28rj5epg
6. Allen M, Frank D, Glen JC, Fardo F, Callaghan MF, Rees G. Insula and somatosensory cortical myelination and iron markers underlie individual differences in empathy. Sci Rep. 2017;3(7):43316. doi: https://doi.org/10.1038/srep43316
7. Decety J. The contribution of forensic neuroscience to psychopathy. Encephale. 2020;46(4):301-307. doi: https://doi.org/10.1016/j.encep.2020.02.007
8. Shamay-Tsoory SG. Inter-brain plasticity underlies empathic learning in social interactions. Front Psychol. 2022;10(13):951248. doi: https://doi.org/10.3389/fpsyg.2022.951248
9. Glas G. Conceptual issues in neuroscientific research on empathy. Int J Law Psychiatry. 2019;65:101358. doi: https://doi.org/10.1016/j.ijlp.2018.05.006
10. Díaz-Narváez VP, Calzadilla-Núñez A, Alonso LM, Torres-Martínez PA, Cervantes Mendoza M, Fajardo-Ramos E. Empathy and Ontogeny: A Conceptual Approach. West Indian Mes J. 2017;66(3):1-4. doi: https://doi.org/10.7727/wimj.2016.344
11. Alderman EM, Breuner CC, Grubb LK, Powers ME, Upadhya K, Wallace SB, et al. Unique Needs of the Adolescent. Pediatrics [Internet]. 2019 Dec 1;144(6). doi: http://dx.doi.org/10.1542/peds.2019-3150
12. Jensen SKG, Tofail F, Haque R, Petri WA Jr, Nelson CA 3rd. Child development in the context of biological and psychosocial hazards among poor families in Bangladesh. PLoS One. 2019;6;14(5):e0215304. doi: https://doi.org/10.1371/journal.pone.0215304
13. Leyton A. A latent class analysis to identify how patterns of Intimate Partner Violence Influence Early Childhood Development outcomes in Honduras. Child Abuse Negl. 2020;107:104609. doi: https://doi.org/10.1016/j.chiabu.2020.104609
14. Almutairi S, Scambler S, Bernabé E. Family functioning and dental caries among preschool children. J Public Health Dent. 2022;82(4):406-414. doi: https://doi.org/10.1111/jphd.12475
15. Olson DH, Russell CS, Sprenkle DH. Circumplex model of marital and family systems: VI. Theoretical update. Family Process. 1983;22(1):69-83. doi: https://doi.org/10.1111/j.1545-5300.1983.00069.x
16. Couture S, Fernet M, Hébert M. A cluster analysis of dynamics in adolescent romantic relationships. J Adolesc. 2021;89:203-212. doi: https://doi.org/10.1016/j.adolescence.2021.04.012
17. Zegers B, Larraín EM, Polaino-Lorente A, Trapp A, Diez I. Validez y confiabilidad de la versión española de la escala de Cohesión y Adaptabilidad Familiar (CAF) de Olson, Russell & Sprenkle para el diagnóstico del funcionamiento familiar en la población chilena. Rev Chilena de Neuro-Psiquiatría. 2003;41(1):39-54. doi: https://doi.org/10.4067/S0717-92272003000100006
18. Díaz-Narváez VP. En Metodología de la Investigación Científica y Bioestadística para Profesionales y Estudiantes de Ciencias de la Salud. Primera Edición. El Salvador: Editorial UEES;. 2019.
19. Martínez-Pampliega A, Castillo II, Vázquez MS. Validez estructural del FACES-20-Esp : Versión española de 20 ítems de la Escala de Evaluación de la Cohesión y Adaptabilidad Familiar. Revista Iberoamericana de Diagnóstico y Evaluación. 2011;29(1):147-165. Disponible en: https://www.aidep.org/sites/default/files/2018-12/r29art8_1.pdf
20. Zicavo N, Palma C, Garrido G. Adaptation and validation of faces 20-ESP: family functioning awareness in Chillán, Chile. Rev. Latinoam. Cienc. Soc. Niñez Juv. 2012;10(1):219-234. Disponible en: https://tinyurl.com/2bzkztb7
21. Yuan KH, Bentler PM. Three likelihoodbased methods for mean and Covariance structure analysis with nonnormal missing data. Sociol. Methodol. 2000;30(1):165-200. doi: https://doi.org/10.1111/0081-1750.00078
22. Franco-Martínez A, Alvarado JM, Sorrel MA. Range Restriction Affects Factor Analysis: Normality, Estimation, Fit, Loadings, and Reliability. Educ Psychol Meas. 2022;83(2). doi: https://doi.org/10.1177/00131644221081867
23. Grace JB, Irvine KM. Scientist's guide to developing explanatory statistical models using causal analysis principles. Ecology. 2020 Apr;101(4):e02962. doi: https://doi.org/10.1002/ecy.2962
24. Schumacker RE, Lomax RG. A Beginner’s Guide to Structural Equation Modeling. Fourth Edition (4th ed.). Routledge; 2015.
25. Raykov T, Hancock GR. Examining change in maximal reliability for multiple-component measuring instruments. Br J Math Stat Psychol. 2005;58(1):65-82. doi: https://doi.org/10.1348/000711005X38753
26. Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Struct Equ Modeling. 2007;14(3):464-504. doi: https://doi.org/10.1080/10705510701301834
27. Ye P, Ju J, Zheng K, Dang J, Bian Y. Psychometric Evaluation of the Parental Reflective Functioning Questionnaire in Chinese Parents. Front Psychol. 2022;28;13:745184. doi: https://doi.org/10.3389/fpsyg.2022.745184
28. Mardia KV. Measures of multivariate skewness and kurtosis with applications. Biometrika. 1970;57:519-530. doi: https://doi.org/10.2307/2334770
29. Kang H. Sample size determination and power analysis using the G*Power software. J Educ Eval Health Prof. 2021;18:17. doi: https://doi.org/10.3352/jeehp.2021.18.17
30. Staffa SJ, Zurakowski D. Statistical power and sample size calculations: A primer for pediatric surgeons. J Pediatr Surg. 2020 Jul;55(7):1173-1179. doi: https://doi.org/10.1016/j.jpedsurg.2019.05.007
31. Muthén LK, Muthén BO. Mplus User’s Guide. 8th ed. Los Angeles, CA: Muthén & Muthén; 2017.
32. Finney SJ, DiStefano C. Nonnormal and categorical data in structural equation modeling. In: Hancock GR, Mueller RO, Editors. Structural equation modeling: A second course. 2nd ed. Charlotte, NC: Information Age Publishing Inc., 2013. p. 439-492.
33. Díaz-Narváez VP, Tierra-Chávez DC, Padilla M, Utsman R, Calzadilla-Núñez A. Declinación en el género y la empatía en alumnos de la Facultad de Odontología de la Universidad Central (Ecuador): Estudio transversal. Rev. Méd. Rosario. 2018;84:55-66. Disponible en: https://pesquisa.bvsalud.org/portal/resource/pt/biblio-1050942
34. Díaz-Narváez VP, Silva-Vetri MG, Calzadilla-Núñez A, López García AL, de la Portilla Lopez A, Reyes-Reyes A. Empathy in professors and students of a school of dentistry in the Caribbean. Pesqui Bras Odontopediatria Clín Integr. 2022;22:e200240. doi: https://doi.org/10.1590/pboci.2022.043
35. Díaz-Narváez VP, Erazo Coronado AM, Bilbao JL, González F, Padilla M, Calzadilla-Núñez C, et al. Reconsidering the 'Decline' of Dental Student Empathy within the Course in Latin America Acta Med Port. 2017;30(11):775-782. doi: https://doi.org/10.20344/amp.8681
36. Díaz-Narváez V, Miranda-Carreño F, Galaz-Guajardo S, Sepúlveda-Navarro W, Zúñiga-Mogollones M, Calzadilla-Núñez A, et al. Variabilidad empática en estudiantes de odontología. Consecuencias aún no entendidas en América Latina. Rev. Fac. Med. 2022;70(1):e91207. doi: https://doi.org/10.15446/revfacmed
37. Díaz-Narváez VP, Bilbao JL, Estrada-Méndez N, Ulloque J, Calzadilla-Núñez A, Barrera-Gil D. Consideraciones sobre la declinación empática en estudiantes de medicina en Latinoamérica. Rev. Cienc. de la Salud. 2020;18(2):1-16. doi: https://doi.org/10.12804/revistas.urosario.edu.co/revsalud/a.9258
38. Ameh PO, Uti OG, Daramola OO. Empathy among dental students in a Nigerian institution. Eur J Dent Educ. 2019;23(2):135-142. doi: https://doi.org/10.1111/eje.12412
39. Schmidt V, Barreyro JP, Maglio AL. Escala de evaluación del funcionamiento familiar FACES III: ¿Modelo de dos o tres factores? Escritos de Psicología - Psychological Writings. 2010;3(2):30-36. doi: https://doi.org/10.24310/espsiescpsi.v3i2.13339
40. Ponce ER, Gómez FJ, Terán M, Irigoyen Coriad E, Landgrave Ibáñez S. Validez de constructo del cuestionario FACES III en Español (México). Atencion Primaria. 2002;30(10):624-630. doi: https://doi.org/10.1016/S0212-6567(02)79124-5
41. Bazo-Álvarez JC, Bazo-Alvarez OA, Aguila J, Peralta F, Mormontoy W, Bennett IM. Psychometric properties of the third version of family adaptability and cohesion evaluation scales (faces-III): A study of Peruvian adolescents. Rev Peru Med Exp Salud Publica. 2016:33(3):462-470. doi: https://doi.org/10.17843/rpmesp.2016.333.2299
42. Dávila Pontón Y, Velez Calvo X, Celleri Gomezcoello A, Aguilera Muñoz J, Díaz-Narváez V, Calzadilla-Núñez A, et al. Empathy and Family Functioning in Medical Students of the University of Azuay, Cuenca, Ecuador. Salud Uninorte. 2020;36(3):571-586. doi: https://dx.doi.org/10.14482/sun.36.3.152.41
43. Duran E, Padilla M, Utsman R, Reyes-Reyes A, Calzadilla-Núñez A, Díaz-Narváez V. Analysis of the relationship between empathy and family functioning in dentistry students of the Latin American University of Science and Technology (ULACIT), San José, Costa Rica. Proceedings of EDULEARN 17 Conference 3rd-5th July 2017, Barcelona, Spain. doi: https://dx.doi.org/10.21125/edulearn.2017.0816
44. Olson DH, Sprenkle DH, Russell CS. Circumplex model of marital and family system: I. Cohesion and adaptability dimensions, family types, and clinical applications. Fami. Process 1979;18(1):3-28. doi: https://doi.org/10.1111/j.1545-5300.1979.00003.x
45. Fan J, Ni X, Wang Y, Qian Y, Li X, Geng Y. Parent-Child Discrepancies in Perceived Parental Emotion Socialization: Associations with Children's Internalizing and Externalizing Problems in Chinese Families. J Youth Adolesc. 2022 Nov 24. 52: 547-560. doi: https://doi.org/10.1007/s10964-022-01711-4
46. Wu W, Ma X, Liu Y, Qi Q, Guo Z, Li S, et al. Empathy alleviates the learning burnout of medical college students through enhancing resilience. BMC Med Educ. 2022;22(1):481. doi: https://doi.org/10.1186/s12909-022-03554-w
47. Brown MEL, MacLellan A, Laughey W, Omer U, Himmi G, LeBon T, et al. Can stoic training develop medical student empathy and resilience? A mixed-methods study. BMC Med Educ. 2022 May 3;22(1):340. doi: https://doi.org/10.1186/s12909-022-03391-x
48. Cao X, Chen L. Relationships between resilience, empathy, compassion fatigue, work engagement and turnover intention in haemodialysis nurses: A cross-sectional study. J Nurs Manag. 2021;29(5):1054-1063. doi: https://doi.org/10.1111/jonm.13243
49. Morel-Barrios M, Díaz-Reissner C. Nivel de empatía en estudiantes de odontología de una universidad paraguaya durante la atención a pacientes en el marco de la pandemia por COVID-19, 2021. Rev. Nac. (Itauguá). 2022;14 (1):018-029. doi: https://doi.org/10.18004/rdn2022.jun.01.018.02
50. Rionda IS, González JVG, Granda FJ, Richaud M, Mestre MV, Lemos V, et al. La influencia de la cultura en los estilos parentales en contextos de vulnerabilidad social. Av. en Psicol. Latinoam. 2013;31(2):419-431. Recuperado de: https://www.redalyc.org/articulo.oa?id=79928611009
51. Calzadilla-Núñez A, Díaz-Narváez VP, Dávila-Pontón Y, Aguilera-Muñoz J, Fortich-Meza N, Aparicio-Marenco, et al. Erosión empática durante la formación médica según el género. Estudio transversal. Arch Argent Pediatr 2017;115(6):556-561. doi: http://dx.doi.org/10.5546/aap.2017.556