
The Use of Physical Screening Tools to Identify Injury Risk Within Pre-Professional Ballet Dancers: An Integrative Review
El uso de herramientas de cribado física para identificar el riesgo de lesiones en los bailarines de ballet preprofesionales: Una revisión integradora
Niall MacSweeney , Charles Pedlar, Daniel Cohen, Ryan Mahaffey, Phil Price
Abstract
Objective: To conduct an integrative review of all relevant research investigating the physical risk factors for injury within pre-professional ballet dancers, to provide insight that may benefit practitioners within these institutions and highlight areas for future research within this specialised population.
Design: Studies were identified from the following electronic databases: MEDLINE via PubMed, SPORTDiscus via EBSCOhost, and Web of Science Core Collection via Web of Science. 8,415 titles were identified during the electronic search process. Five studies satisfied the inclusion criteria and were included in the review. The modified Agency for Healthcare Research and Quality (AHRQ) scale for observational studies was used to assess study quality.
Results: The review identified that the following physical characteristics may influence prospective injury risk in pre-professional ballet dancers: age and maturation status, anthropometrics and body composition, strength and power, joint mobility and range of motion, specific dance function, and cardiorespiratory fitness.
Limitations: The research identified lacked methodological quality. This, combined with the low number of studies identified, makes the design of screening protocols challenging for practitioners.
Originality: Despite the number of pre-professional balletic institutions worldwide, previous reviews have not used a systematic search strategy or investigated both sexes in this cohort. Due to the unique demands of ballet, an understanding of the interaction between injury and physical characteristics is a critical step in order to reduce injury burden.
Conclusions: This review succeeded in determining risk factors for injury within this population, but, due to insufficient evidence, could not provide robust screening recommendations.
Keywords
Dance; Injuries; Risk Factors; Ballet; Pre-Professional; Review; Adolescent; Screening; Biomechanics; Physiology.
Resumen
Objetivo: Llevar a cabo una revisión integradora de toda la investigación relevante sobre los factores de riesgo físico de las lesiones en los bailarines de ballet preprofesionales, para proporcionar una visión que pueda beneficiar a los profesionales de estas instituciones y resaltar las áreas para futuras investigaciones en esta población especializada.
Diseño: Los estudios se identificaron en las siguientes bases de datos electrónicas: MEDLINE vía PubMed, SPORTDiscus vía EBSCOhost y Web of Science Core Collection vía Web of Science. Se identificaron 8.415 títulos durante el proceso de búsqueda electrónica. Cinco estudios cumplieron los criterios de inclusión y se incluyeron en la revisión. Para evaluar la calidad de los estudios, se utilizó la escala modificada de la Agency for Healthcare Research and Quality (AHRQ) para estudios observacionales.
Resultados: La revisión identificó que las siguientes características físicas pueden influir en el riesgo prospectivo de lesiones en los bailarines de ballet preprofesionales: edad y estado de maduración, antropometría y composición corporal, fuerza y potencia, movilidad articular y amplitud de movimiento, función específica de la danza y aptitud cardiorrespiratoria.
Limitaciones: La investigación identificada carecía de calidad metodológica. Esto, combinado con el bajo número de estudios identificados, hace que el diseño de protocolos de detección sea un reto para los profesionales.
Originalidad: Las revisiones anteriores no han utilizado una estrategia de búsqueda sistemática ni han investigado ambos sexos en esta cohorte. Debido a las exigencias únicas del ballet, la comprensión de la interacción entre las lesiones y las características físicas es un paso fundamental para reducir la carga de lesiones.
Conclusiones: Esta revisión logró determinar los factores de riesgo de lesiones dentro de esta población, pero, debido a la insuficiencia de evidencia, no pudo proporcionar recomendaciones sólidas de cribado.
Palabras clave
Danza; Lesiones; Factores de Riesgo; Ballet; Preprofesional; Revisión; Adolescente; Detección; Biomecánica; Fisiología.
Introduction
Ballet dancers specialise in ballet from an early age and enter pre-professional training schools from as young as ten years old [1]. Whilst in these ballet schools, dancers train extensively alongside academic study to obtain sufficient physical and technical mastery to reach the professional level. They also mature and change physically during this intense training period [2-5]. Ballet is physically demanding, with dancers required to achieve high levels of neuromuscular control in extreme ranges of motion with performances punctuated by high-intensity activities such as jumping and turning [6]. These demands expose dancers to a significant risk of injury [7,8] which occur primarily in the lower extremities, in particular, the knees, ankles, and feet [9,10] and are predominantly overuse in nature. Injury risk may be increased for young dancers who attend pre-professional schools, due to the greater exposure to high training loads compared to recreational dancers of a similar age [5,11]. The reported injury incidence in this population varies within the literature; between 0.77 to 3.52 incidents per 1000 hours of training [9,12].
As retaining a place within pre-professional dance institutions is performance-dependent and competitive, time loss from training due to injury can negatively impact technical development and professional success [4,10,13,14] as well as health. Therefore, identifying physical characteristics of dancers that may be at a heightened injury risk can help to inform intervention strategies. For instance, Pilates or strength and conditioning sessions are modes of training that can be or are integrated into, so they may influence the physical condition of the dancers and could consequently impact upon injury incidence [6,15,16]. Risk factor identification in this area is therefore crucial in informing the design of screening practices and guiding the practitioner towards conditioning methodologies that may subsequently be implemented in dancers who present with these factors. It is also important to inform the design of research which needs to be implemented to allow robust recommendations to be provided to practitioners.
Screening is commonly used in practice to identify risk factors associated with injury risk [17]. However, there is a lack of consensus in the research over which factors to examine and how to effectively screen for these qualities, as practitioners have questioned the value of conducting injury risk screening [18]. To allow practitioners to implement screening strategies effectively and understand their value, the research must provide clear guidance to implement effective specific screening procedures for this unique population. It is also important that the methodological quality and limitations of existing research is examined, so that researchers can critically evaluate current screening protocols to inform future study design and expand upon the available literature.
Systematic reviews have focused on injury risk factors within dance [17,19,20], aesthetic sports [21] and pre-professional dancers of varying styles [14]. Due to the unique demands of ballet such as performing “en pointe” (dancing with the feet fully plantarflexed and using blocks in the shoes to support balance) and in a “turned out” position (with hips in external rotation), general dance/aesthetic sports research may not be applicable to a pre-professional ballet dancer. Bowerman et al. [22] conducted a narrative review investigating risk factors for lower limb injury within elite pre-professional female ballet dancers. They concluded that physical fitness characteristics, such as strength and mobility, and genetic/epigenetic factors, like growth and maturation status, should be investigated alongside dance specific movement strategies to evaluate an individual’s injury risk. An integrative review can expand on this by using a more systematic search strategy focused on the population of interest to provide more specific guidelines to both researchers and practitioners.
This study aimed to undertake an integrative review of the literature that examined prospective injury risk factors in pre-professional ballet dancers, aiming to provide practitioners with guidance to identify risk factors and the screening methods used to assess these factors. Furthermore, it will highlight areas for future research to guide the design of potential screening and intervention protocols in the future.
Methods
An integrative review search process was conducted, following the methodological guidelines of Whittemore et al. [23].
Search Process
Studies were identified from the following electronic databases: MEDLINE via PubMed, SPORTDiscus via EBSCOhost and Web of Science Core Collection via Web of Science. The full search list of search terms can be found in Table 1. The specific strategy and pattern of searches conducted from the 28th of October 2020 can be seen in Table 2.
Table 1. List of search terms and groups
| Group A-Activity | Group B-Population | Group C-Injury | Group D-Risk | ||||
|---|---|---|---|---|---|---|---|
| PM | WS/SD | PM | WS/SD | PM | WS/SD | PM | WS/SD |
| Dance [MeSH] | Danc* | Adolescent [MeSH] | Adolescen* | Wounds and Injuries [MeSH] | Injur* | Risk Factors [MeSH] | Risk |
| Ballet | Ballet | Pre-Professional | Pre-Professional | Athletic Injuries [MeSH] | Risk Assessment [MeSH] | Risk Assessment | |
| Pre Professional | Pre Professional | Screen* [tw] | Risk Factors | ||||
| Preprofessional | Preprofessional | Profil* [tw] | Screen* | ||||
| Elite | Elite | Predic*[tw] | Profil* | ||||
| Correlat*[tw] | Predic* | ||||||
| Correlat* | |||||||
Note. 1. All terms combined in search with OR.
Note: 2. Key: PM- PubMed (MEDLINE), WS- Web of Science (Web of Science Core Collection), SD- EBSCO Host (SPORTDiscus).
Table 2. Full electronic search strategy
| Search Strategy | PM | WS | SD | |
|---|---|---|---|---|
| Preliminary Searches | 1) A | |||
| 2) A AND B | ||||
| 3) A AND C | ||||
| Searches used for Data Synthesis | 4) 2 AND C | 30/11/2020 | 1/12/2020 | 2/12/2020 |
| 5) 1 AND D | 8/12/2020 | 14/12/2020 | 8/12/2020 | |
| 6) 2 AND D | 20/12/2020 | 20/12/2020 | 21/12/2020 | |
| 7) 3 AND D | 28/10/2020 | 8/11/2020 | 27/11/2020 |
Note. Key: PM- PubMed (MEDLINE), WS- Web of Science (Web of Science Core Collection), SD- EBSCO Host (SPORTDiscus).
Inclusion/exclusion criteria
Inclusion criteria were as follows: 1) original experimental research; 2) written in English; 3) investigating full time pre-professional ballet dancers; 4) investigating physical characteristics and prospective associations with injury risk. Studies were excluded if they 1) were conference posters or proceedings, 2) included dancers who were only attending summer schools and not in full time programs, 3) investigated dancers who took part in balletic training as part of a wider dance curriculum, or if dancers that specialised in ballet were indistinguishable in the reporting of results from other dancers, and 4) investigated physical screening tools that were considered invasive (e.g., blood tests were considered too invasive and therefore unlikely to occur in a standard screening review).
Data Collection
Following the initial searches, titles were screened (by author NM) using the eligibility criteria outlined above. Abstracts were then screened for potential inclusion. Additionally, reference lists were searched for additional studies not identified during the electronic database search. This process was then repeated to screen the remaining full texts before data extraction. A second independent reviewer (PP) replicated this process from the abstract stage, and the results were compared before the final study inclusion was agreed upon. Where there was no agreement, the wider research team (RM, DC and CP) was consulted, and a consensus was reached on inclusion.
Data Synthesis and Risk of Bias
Methodological quality assessment was completed independently by two authors (NM and PP) following the same method. Disagreements were discussed and resolved by consensus within the wider research team (RM, DC, and CP). Research quality and risk of bias were assessed using the modified Agency for Healthcare Research and Quality (AHRQ) scale for observational studies [24-27]. Criteria for grading was used based on the 1) study question (2 points), 2) study population (8 points), 3) comparability of subjects (22 points), 4) exposure or intervention (11 points), 5) outcome measures (20 points), 6) statistical analysis (19 points), 7) results (8 points), 8) discussion (5 points), and 9) funding or sponsorship (5 points). A total quality score out of 100 was then calculated for each study [24]. Any differences in scoring from the first two reviewers were discussed and further analysed with the wider research team (RM, DC, and CP) to gain consensus. Full scoring criteria can be found in Appendix.
Results
In total 8,415 sources were identified during the electronic search process, reduced to 5,113 titles following the removal of duplicates, which were screened for eligibility. After the screening of abstracts, 25 studies were identified for full-text review from the initial identification process. A further 2 studies were identified from searching the reference lists of the selected abstracts. Of the 27 full texts, 5 were identified as fitting the selection criteria (Figure 1 [28]). In total 737 students were investigated in the studies. Study participant numbers varied from n=13 to n=359 with subject ages ranging from 9 years old to 19 years old. Study characteristics can be found in Table 3.
Fifure 1. Preferred reporting items for systematic review and meta-analyses (PRISMA) literature search flow diagram
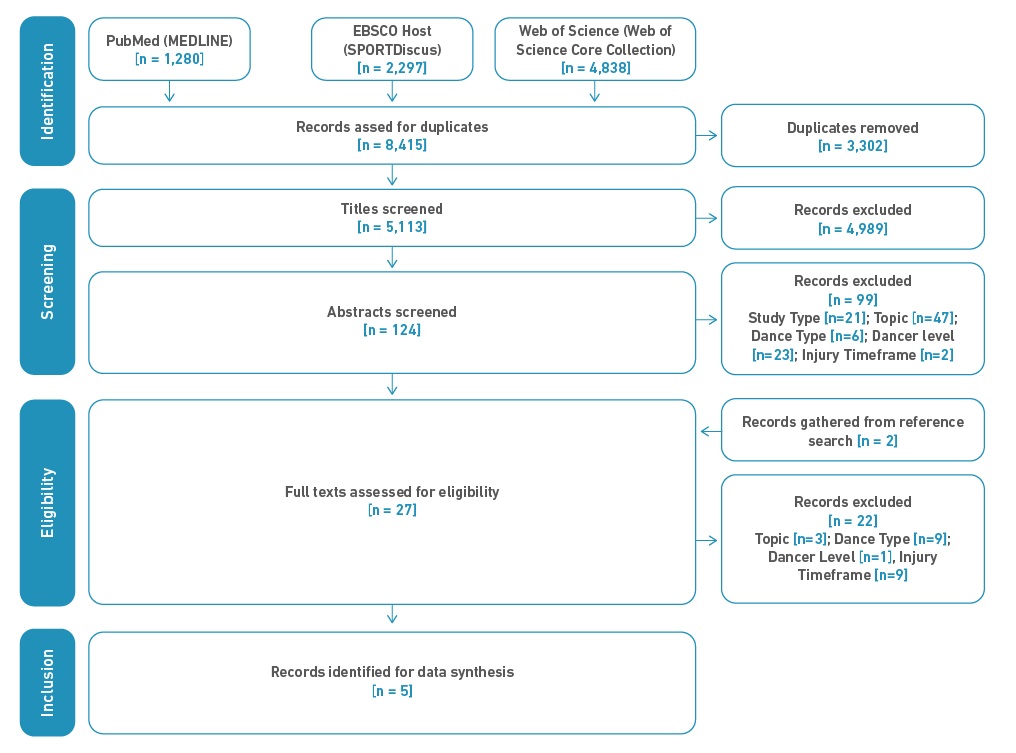
Table 3. Study Characteristics
| Author | Population Description | N of Participants | Gender of Participants | Age of Participants (as reported) | Country of Training | N of Injuries | Injury Type Examined | Study Design | Injury Definition | Study Time Period | Students Training Schedule (as reported) | Risk Factor Examined |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Twitchett et al. 2010 [31] | Elite Vocational Ballet Students | 13 | Female | 19 ± 7 | Britain | 11 | All | Cohort Study | A physical or psychological problem deriving from stress or other causes to do with performance, rehearsal, training, touring or the circumstances of dance life | 15 weeks | 1 class and 2 rehearsals daily on top of performances | Anthropometry and Body Composition, Strength and Power, Joint Mobility and ROM, Cardiorespiratory Fitness |
| Bowerman et al. 2014 [22] | Elite Adolescent Ballet Dancers (Australian Ballet School) | 46 | Mixed (29 female, 13 male) | 16 ± 1.58 | Australia | 59 | All | Cohort Study | Any physical harm resulting in pain or discomfort that required a dancer to modify their dance activity during one or more classes or cease all class | 6 months | 19 hours per week | Age and Maturation Status, Specific Dance Function |
| Rudavsky et al. 2018 [29] | Young Ballet Dancers (Australian Ballet School and Victorian College of the Arts Secondary School) | 57 | Mixed (34 female, 23 male) | 11-18 years | Australia | 5 | Patellar tendinopathy | Cohort Study | Tendon pathology diagnosed on ultrasound scan | 2 years | 4-8 hours per day | Age and Maturation Status |
| Gamboa et al. 2008 [12] | Elite Preprofessional Ballet School Students | 359 | Mixed (288 female, 71 male) | 9 to 20 years | United States of America | 151 | All | Cohort Study | Any pain or discomfort requiring treatment from a physiotherapist | 5 years (annual analysis) | 20 hours ballet, 2 hours cross training/Pilates per week | Age & Maturation Status, Strength and Power, Joint Mobility and ROM, Specific Dance Function |
| Leanderson et al. 2012 [30] | Young Swedish Ballet Dancers (Royal Swedish Ballet School) | 262 | Mixed (130 female, 86 male) | 9 to 21 years old | Sweden | 216 | All | Cohort Study | Any pain or discomfort requiring treatment from an orthopaedic specialist | 7 years | 6-11 hours per week | Hypermobility |
Results of Synthesis and Risk of Bias
Table 4 shows the research quality assessment data per study. Gamboa et al. [12] achieved the lowest score (40/100), whereas the Rudavsky et al. [29] study scored the highest of the studies assessed on all listed criteria (58/100). The research of Leanderson et al. [30] was presented as a section of a thesis; therefore, isolating the introduction and discussion was particularly challenging. To address this, the research team agreed to remove 20 points from the potential total score for this research in areas where data was lacking due to the format of the research and a fair comparison could not be made (see Table 4). Based on the format of the research, the researchers concluded that it had undergone a less rigorous review process and therefore did not justify as high a score as the other studies included in this review. Overall, studies achieved the highest quality score in the discussion section. In contrast, there was a lack of comparability of the subjects recruited within each trial and the studies generally did not acknowledge funding and sponsorships sufficiently and consequently scored poorly in these areas.
Table 4. Research Quality Assessment Criteria
| Study | Study Question | Study Population | Comparability of Subjects | Exposure or Intervention | Outcome Measures | Statistical Analysis | Results | Discussion | Funding and Sponsorship | Total Score |
|---|---|---|---|---|---|---|---|---|---|---|
| Marks available | 2 | 8 | 22 | 11 | 20 | 19 | 8 | 5 | 1 | 100 |
| Twitchett et al., 2010 [31] | 1 | 3 | 7 | 7 | 12 | 9 | 0 | 5 | 0 | 45 |
| Bowerman et al., 2014 [22] | 1 | 6 | 6 | 7 | 13 | 9 | 4 | 5 | 0 | 51 |
| Rudavsky et al., 2018 [29] | 2 | 5 | 6 | 9 | 13 | 14 | 4 | 5 | 0 | 58 |
| Gamboa et al., 2008 [12] | 2 | 6 | 4 | 0 | 13 | 5 | 6 | 4 | 0 | 40 |
| Leanderson et al., 2012 [30] | 0 (0) | 5 (5) | 5 (19) | 9 (10) | 9 (19) | 8 | 4 | 0 (0) | 0 (0) | 40 |
Note. Key: ()- Marks available for study due to formatting..
The selected studies’ findings are presented around major themes of injury risk, which emerged from the integrative review: age and maturation status, anthropometric and body composition, strength and power, joint mobility and ROM, specific dance function, and cardiorespiratory fitness.
Age and Maturation
Age and maturation status were investigated in three studies. Both Gamboa et al. [12] and Bowerman et al. [22] did not find an association between chronological age and injury risk and no significant differences in sexual maturation (age at onset of menarche (AoM)) were observed between injured and non-injured female dancers. Rudavsky et al. [29] found that maturation level as estimated using the Mirwald calculation of proximity to peak height velocity was not significantly related to symptomatic patellar tendon pathology. Bowerman et al. [22] also found only unclear (greater than a 5% chance the true value of the rate ratio could substantially increase and decrease) links between injury risk and maturation assessed using the Tanner scale method, but did find that a another measure of maturity -a change of over 0.5 cm in right foot length- was associated with a moderately likely increase in injury risk (Rate Ratio [RR] = 1.41; Confidence Interval [CI]: 0.9-2.1).
Anthropometric and body composition measurements
The majority of studies collected anthropometric measurements as part of their descriptive data for the participants. However, only two of the studies looked at the interaction between anthropometric/body composition variables and injury risk. Twitchett et al. [31] found that dancers with a lower body fat percentage had a higher severity of injuries. Bowerman et al. [22] found unclear (RR = 1.08, CI: 0.85 - 1,37) associations between body mass and injury risk.
Strength and power
Two studies examined associations with measures of muscular strength and power. Twitchett et al. [31] found no association between injury risk or injury severity and “lower body power” -defined as jump height in a ballet specific turned-out position. Gamboa et al. [12] also investigated the upper body, core, and scapular control, but found no significant difference between those who suffered future injury and those that did not. However, a composite lower body strength score calculated using a combination of manual muscle testing scores across 16 different lower body movements revealed that a significantly reduced injury risk in the stronger dancers (injured score = 4.4 ± 3.0, non-injured score = 4.5 ± 0.3).
Joint Mobility and ROM
Several studies assessed joint mobility through a range of methods. Joint mobility can be measured statically, passively, and actively. Static assessments of posture were conducted by Gamboa et al. [12], identifying that dancers who sustained an injury in the following year were 74% more likely to display excessive right foot pronation in these tests than non-injured dancers (RR=1.74). Indicators of hypermobility or joint laxities, such as knee hyperextension and the knee integrity score, were not significantly associated with injury risk. In contrast, hypermobility was assessed directly by Leanderson et al. [30] and students were categorised as normal, hypermobile, or as displaying generalised joint laxity (GJL). Students with GJL displayed a significantly greater injury risk than hypermobile or normal students. Leanderson et al. [30] also found that this risk was greater in older students. Gamboa et al. [12] assessed passive joint ROM in ankle plantarflexion, dorsiflexion, hip external, and internal ROM, as well as in the quadriceps, hamstrings, hip flexors, latissimus dorsi, and pectoralis major. Low levels of ankle plantar flexion on the right leg were associated with a significant increase in injury risk (Risk Ratio [RiR] = 1.50). Twitchett et al. [31] also assessed passive lower extremity flexibility in an assisted développé position, but found no significant correlations with injury risk or severity.
Specific Dance Function
Four of the studies assessed active mobility using a two-dimensional analysis of ballet specific positions. Bowerman et al. [22] analysed pelvic angle and knee angle both in the temps levé and the fondu across both legs, finding that a decreased knee valgus angle of 10◦ during the right leg fondu indicated a likely decreased injury risk (RR = 0.68, CI: 0.5 - 1) and that a reduced pelvic tilt angle on the right leg also displayed a likely decreased injury risk (RR = 1.28 CI: 0.9 - 1.8). During the temps levé, an increased pelvic tilt angle on the left leg also indicated a likely reduction in injury risk (RR = 0.52, CI: 0.3 - 0.9) and there was a small decrease in injury risk for an increased knee valgus angle on the right leg (RR=0.72, CI:0.5 - 1). Gamboa et al. [12] assessed functional ROM in a turnout position both on the standing and gesture leg, using a combination of “footprints” and an arthrodial goniometer, and also examined joint alignment in a grand plie in second position. All these tests displayed no significant relationship with injury risk. Twitchett et al. [31] assessed ROM during an active développé position, but did not find any significant correlations with injury risk or severity.
Cardiorespiratory Fitness
Only one study assessed the relationship between cardiorespiratory fitness and injury. Twitchett et al. [31] examined heart rate, following the dance aerobic fitness test (DAFT). They found a significant positive correlation between heart rate at the end of the test (r=.590) and overall injury incidence, but no association with acute injuries.
Discussion
Data Extraction
The present integrative review aimed to investigate potential associations between physical characteristics and prospective injury risk for pre-professional ballet dancers. Table 5 shows the main findings of this review with recommendations for future research. Only 5 studies met our inclusion criteria, demonstrating a scarcity of both population specific and high-quality research. During the final full-text review stage, the primary reason for exclusion was due to studies not distinguishing between ballet dancers and other dance styles. This is problematic, as ballet training involves unique movements and characteristics that combine to produce a training load that is not replicated in other dance styles [32,33]. The other key reason for exclusion was that many of the studies identified were cross-sectional or retrospective and therefore did not examine injury risk prospectively. Within the five studies, a large number of potential injury risk factors are assessed, demonstrating the notion that injury risk is multifactorial for young dancers. This complexity, combined with the limited evidence available, reaffirms the challenges for practitioners working with these dancers.
Table 5. Integrative Review Summary
| Findings | Recommendations for future research |
|---|---|
|
|
Methodological Quality
The modified AHRQ scale identified various areas in which methodological quality was limited. This may have influenced the findings and interpretations of the studies identified. One of the key areas that the studies performed badly on was the comparability of subjects. For instance, none of the studies matched different age groups and the studies that included male and female participants did not have an equal split of genders. Only one study collected medical history before participation in the study and included this as part of the analysis [29]. Moreover, differences in training schedule/repertoire and training experience of the participants were not accounted for in any of the studies. Only one of the studies detailed the subject recruitment process; none of them detailed how they managed data for participants that dropped out from the study or what the criteria for this were. This increases the potential for the characteristics of the participants to influence the study’s findings. This is a particularly important consideration when exploring injury risk in ballet dancers, as the training demands of different genders and dancers performing different pieces can vary significantly [32,34].
Age and Maturation
Three of the studies included assessments of age and maturation, with two studies investigating chronological age and finding no relationship with injury. Of the studies included in this review, Bowerman et al. [22] found a likely increased risk of injury for individuals with a growth rate of more than 0.5 cm in the right foot during a six-month period. This measure of increase in the length of the bones was used as a marker of maturation. However, this methodology can be questioned as validation studies have not been performed in adolescents [35].
Both Gamboa et al. [12] and Bowerman et al. [22] assessed associations with sexual maturation. Gamboa et al. [12] investigated AoM but did not find any significant interactions with injury risk. However, assessing the menstrual cycle may be less reliable in adolescent dancers with later AoM and an irregular menstrual pattern observed in these populations [36-38]. The Tanner scale used by Bowerman et al. [22] does provide a reliable assessment of sexual maturation [39], although their analysis, which involved grouping the students using Tanner stages, may have some limitations. For example, stages two and three were classified as “less mature” and four and five as “more mature”. This may have limited the sensitivity of these measures and the ability to detect associations, since large changes can occur in relatively small-time frames, which may increase injury risk. For instance, stages 4 and 5 were placed together, which typically represents 2 to 3 years of development in which both peak height and weight velocity may occur.
Rudavsky et al. [29] used the Mirwald method [40] to estimate proximity to peak height velocity and found no correlation with tendon pathology. However, these findings should be treated with caution due to the limited number of participants and because the Mirwald maturity offset calculations may be unreliable in later and earlier developers [41]. Alternative methods to predict the stage of maturation, such as the Khamis-Roche method, have been widely adopted in other adolescent sporting contexts, which have been shown to display a lower error rate [42] and could therefore provide a useful alternative for future research.
Interestingly, none of the studies reported longitudinal growth in stature to indicate maturation levels, which presents a reliable, non-invasive technique for understanding maturation levels. Bowerman et al. [22] collected results over six months and Gamboa et al. [12] only used the first year of assessment for each participant and acute changes in growth patterns that could lead to heightened injury risk may therefore have been difficult to collect during this timeframe [43]. Rudavsky et al. [29] collected data for two years and used measurements of stature as part of the Mirwald maturity offset calculations, but changes in stature was not investigated. Inclusion and analysis of more longitudinal measures of changes in growth in future research would assist in conducting analysis around maturation levels.
Despite the inconclusive findings in the reviewed literature, all the researchers suggested more detailed investigation with more participants and longitudinal measures of maturation related changes that might provide a better insight. The wider literature provides the rationale for this, whereby injuries affecting the apophysis, which are directly influenced by adolescent growth and maturation [44,45], are often identified within pre-professional dancers [5]. Incidence could therefore potentially be reduced by managing dancers during periods when dancers are at heightened risk. Despite the complexities of analysing these factors, this area also warrants further investigation due to the potential influence maturation may have on modifiable physical risk factors, which may mediate injury risk such as strength and ROM [46]. For example, Kolokythas et al. [46] found that male pre-professional dancers showed age related increases in jump height whereas female dancers did not. This was accompanied by an age-related increase in injury incidence in the female dancers. This might indicate a mediating effect of male puberty on muscle characteristics and therefore injury. The measurement of longitudinal changes in size and physique, alongside sexual maturation, is required to understand how adolescent maturation can be accurately assessed and provide further insight into potential injury mechanisms.
Anthropometric and Body Composition Measurements
Ballet dancers typically have slender physiques with low body fat [47]. Individuals that have the lowest body fat percentages within this cohort may therefore be at risk of having an unhealthy body composition that may increase the risk of injury [48]. Associations between injury risk and anthropometric and body composition variables were investigated in two studies, one of these observing significant results. Twitchett et al. [31] found dancers with a lower body fat percentage had significantly increased injury severity (r=-0.614). The limited number of injuries (n=8) observed prevented an analysis of incidence and means findings may need confirming in larger cohorts before generalising to all ballet dancers. However, these findings are somewhat supported by the work of Benson et al. [49], who investigated the links between Body Mass Index (BMI) and injury in young professional ballet dancers and found that dancers with a BMI of 19 or lower were more time-restricted from dance through injury. Nevertheless, as BMI can be influenced by both lean body mass and fat mass these findings could also be linked to a lack of muscle and therefore strength.
For the practitioner, anthropometric information can be obtained with varied levels of detail and ease. Sophisticated measures such as Dual-energy X-ray absorptiometry can identify bone density, lean body mass, and body fat percentage, but are expensive, and expose dancers to radiation. These can be contrasted with measurements of height and weight collected using a stadiometer and scales, which can be easily obtained but lack precision. A wide variety of these measures have been recommended by the researchers both in this review [11,31] and in the wider dance literature [49-51], due to their potential to identify dancers with inadequate energy availability [52]. This link between energy consumption, body weight and injury has been indicated by Frusztajer et al. [51] in professional ballet dancers, who found that, after controlling for age, weight, and height, dancers that consumed less energy and had weight fluctuations that dropped to a lower percentage of ideal body weight, had a higher incidence of stress fractures. This study was also interesting in that it investigated longitudinal changes in body weight as well as current anthropometric status, which could provide further insight if adopted with pre-professional dancers. Despite the potential benefits these measures might provide, due to the heightened risk of eating disorders and body consciousness among dancers [53], examining anthropometric and body composition factors may present an ethical dilemma for a practitioner, so appropriate care safeguarding should be taken before considering the investigation of these factors or inclusion in screening processes.
Strength and Power
Overuse injuries are the most common mechanism for injury among pre-professional ballet dancers [9,10]. Despite the evidence that increasing force production capabilities may be effective in reducing the risk of overuse injuries in athletic activity [54], we found only two studies that examined relationships between strength or power and injury risk. A total of 6 strength measures were taken across the two studies. However, the only significant finding was that lower manual muscle testing across a range of lower body movements was related to injury risk [12]. Balletic injuries primarily occur in the lower body. Upper body and trunk strength measures examined in these studies may therefore not correspond with these types of injuries, suggesting screening lower body strength may be more valuable for practitioners [9,10,12]. Despite this, the use of manual muscle testing has been questioned in the literature due to a lack of sensitivity [55,56] and intra-tester reliability [57]. Moreover, there is a lack of ecological validity when using manual muscle testing, as the positions in which an individual muscle group is tested do not replicate the multi-joint nature of dancing or the muscle activation patterns for the specific muscle groups tested. Measurement of lower extremity biomechanics during more dynamic assessments of dance movements using equipment such as force plates, 3D motion capture, and Inertial Measurement Units (IMU) may enable practitioners to examine dance in a more specific context. These techniques can be utilised to combine standardised measures of strength and power assessments with more dynamic dance activity.
Twitchett et al. [31] attempted to investigate a correlate of power output in a more ballet specific context by measuring height achieved in a ballet specific jump, but found no relationship with prospective injury risk. Jumping using ballet specific techniques may modify jump strategy and limit dancers' ability to express their maximum physical output [58], which may have influenced this finding of no relationship between jump height and injury risk. It may be more appropriate when measuring a physiological capacity, such as power or force output, to use measurement strategies that have been used consistently and validated in the wider scientific literature. Analysis of these recognised qualities can then be cross validated with dance specific movements using more bespoke equipment for biomechanical analysis, such as those listed in the preceding paragraph. This enables researchers and practitioners to determine relationships between these underlying capacities and performance in dance specific activities, thus providing a more holistic analysis of how various capacities influence dance performance and injury risk.
Joint Mobility and ROM
To achieve the desired aesthetic of ballet performance, dancers must have high levels of joint mobility and move through an extreme ROM. Briggs et al. [59] suggest that while the ability of hypermobile dancers to achieve extreme ROM may benefit dance aesthetic, these dancers are more likely to suffer from more severe injuries and incur a greater number of tendon injuries, a concept corroborated by Leanderson et al. [30]. General Joint Laxity (GJL) has been linked to various neurophysiological deficits that can affect proprioception, joint stability, inflammatory response, and psychology [60]. However, the range and manifestation of these deficits differ significantly between individuals [61]. Furthermore, hypermobility assessment criteria such as the Beington assessment tool are not precise enough to identify more complex interactions with physical attributes. Further research is needed to investigate specific relationships between hypermobility, GJL, physical characteristics, and injury due to the prevalence of these conditions within ballet.
Across the studies examining ROM, only passive plantarflexion ROM in the right foot/ankle was identified as having any relationship with injury risk [12]. Plantarflexion is needed to achieve the “pointe” of the foot required in both closed and open chain movements in ballet and is a key aesthetic of balletic performance [62]. Attempting to achieve this position without the passive flexibility to underpin the technique may lead to increased stress on the foot itself or around the structures trying to compensate for this lack of mobility [62,63]. For instance, certain dancers may have bony restrictions such as an os-trigonum or Steida’s process, which might limit the ability to fully plantarflex the foot. This increases the demands on, not just the ankle and foot joints, but also further up the chain, particularly in closed chain positions such as standing “on pointe” [64]. ROM like strength is a small factor of overall functional performance. Due to this, ROM measures should be studied alongside more dynamic dance activities to understand these relationships and identify potential associations with injury risk.
Specific Dance Function
Both Gamboa et al. [12] and Bowerman et al. [22] found associations between postural factors of the turnout position and injury risk. Bowerman et al. [22] examined the temps levé and fondu movements and identified an association between excessive pronation of the foot during those movements and injury. Researchers within ballet have identified that greater foot pronation can be associated with “rolling” the feet and “forcing” turnout, which may then influence injury risk [65]. These turnout positions are unique to ballet and therefore these findings may not be replicated in non-balletic populations. Changes in dance biomechanics may be influenced by changes in limb length, tissue properties, and coordination that can occur during maturation, so this process may exacerbate the impact of these findings.
Despite this, neither Bowerman et al. [22] nor Gamboa et al. [12] replicated these results on the left limb. Interestingly, despite the range of more global measures of turnout examined by Gamboa et al. [12], none showed any relationship with injury risk. Anatomical structure, passive joint mobility, muscular strength, and coordination of all of these elements throughout various ballet movements underpin a dancer’s functional turnout [65,66]. Potentially because of the highly complex interrelationships between these factors and functional performance, researchers have failed to identify screening strategies that accurately measure a dancer’s turnout. Once screening measures have been validated against in-class balletic performance, potential associations between lower limb biomechanics and injury can be explained. Tools, such as IMUs and 3D motion capture, that could allow more dynamic pictures of these relationships should be used so that inter- and intra-individual differences can be explored in the required detail.
Cardiorespiratory Fitness
Twitchett et al. [31] found that dancers with higher DAFT heart rates displayed a higher injury risk. They suggested that this may be explained by a lower fitness level leading to a loss of neuromuscular control whilst dancing resulting in an increase in injury risk. However, these findings are based on a small number of study participants (n = 13) and relatively high number of injuries (n=8), so they should be interpreted with caution. Furthermore, whilst the DAFT is a dance specific test, it is difficult to ascertain how performance in this test replicates responses to daily and weekly ballet training. Longitudinal measures of cardiorespiratory responses to training can be obtained during dance practice, using heart rate and respiratory frequency monitoring devices, and could be used to corroborate the findings of the DAFT and further investigate relationships with injury risk.
Practical implications
Many of the modifiable physical characteristics highlighted by this review may influence one another and interact in various ways with balletic performance to influence injury risk. They are also influenced by non-modifiable factors such as growth, maturation and stature. In addition to the lack of evidence for the associations between each factor and injury risk, there is also a lack of depth in the available research due to the methodologies characterising these factors often being sub-optimal.
Russell et al. [67] suggests that screening for injury risk forms the first of five essential categories for providing effective healthcare provision. Despite this, there is a lack of evidence on how to design effective screening protocols within pre-professional ballet schools and a lack of understanding of how physical characteristics affect dance performance and injury risk. In other elite sporting environments, screening is used in conjunction with performance data to provide a more holistic approach to injury prevention. For instance, within association football, aerobic capacity can be measured during screening [68] and then cross-referenced with a player’s real-time training and match data collected via Global Positioning Systems [69]. This allows practitioners to be proactive in intervention strategies that might reduce injury risk, either by increasing physical capacities or reducing training demands [70]. Despite the elite training requirements of young ballet dancers, there is currently not enough guidance in the literature to develop and apply a similar model.
Limitations
This review was limited in that only five studies were found that matched the inclusion criteria. Furthermore, a wide range of factors were identified and examined, but the specific factors and way they were measures was not consistent across studies and varied methods of data analysis were used. This meant that comparing the studies directly was challenging and robust statistical comparisons of the existing research was therefore not possible.
Conclusion
Despite the rigorous and exhaustive search performed, there is a paucity of research investigating risk factors for injury for pre-professional ballet dancers. This review identified characteristics that may influence prospective injury risk but could not provide specific tools for screening these factors based on current evidence. This presents a challenge for practitioners working within these environments. Various important considerations for further investigation are suggested within this review. For instance, using standardised and replicable screening measures, understanding longitudinal changes in both modifiable and non-modifiable physical characteristics, and investigating how dancers with specific characteristics perform during their regular dance activity.
References
1. Mitchell S. Health and Wellbeing in Elite Female Ballet Dancers: Implications of Maturity Timing. [Internet] [Doctoral Dissertation]. Bath (Somerset): University of Bath; 2018. Available from: https://researchportal.bath.ac.uk/en/studentTheses/health-and-wellbeing-in-elite-female-ballet-dancers-implications-
2. Caine D, Goodwin BJ, Caine CG, Bergeron G. Epidemiological Review of Injury in Pre-Professional Ballet Dancers. J Dance Med Sci. 2015 Nov;19(4):140-8. doi: https://doi.org/10.12678/1089-313X.19.4.140
3. Ekegren C, Quested R, Brodrick A. Epidemiology of Injuries Among Elite Pre-Professional Ballet Students. Br J Sports Med. 2011 Apr;45(4):347-347. doi: https://doi.org/10.1136/bjsm.2011.084038.105
4. Mitchell S, Haase A, Cumming S, Malina R. Understanding Growth and Maturation in the Context of Ballet: A Biocultural Approach. Res Dance Educ. 2017 Sep;18(3):291-300. doi: https://doi.org/10.1080/14647893.2017.1387525
5. Poggini L, Losasso S, Iannone S. Injuries During the Dancer’s Growth Spurt: Etiology, Prevention, and Treatment. J Dance Med Sci. 1999 Jun;3(2):73-9. [online]. Available from: https://www.ingentaconnect.com/content/jmrp/jdms/1999/00000003/00000002/art00006?crawler=true [Accessed 2022 Sep 04].
6. Koutedakis Y, Jamurtas T. The Dancer as a Performing Athlete: Physiological Considerations. Sports Med Auckl NZ. 2004 Feb 1;34:651-61. doi: https://doi.org/10.2165/00007256-200434100-00003
7. Allen N, Nevill AM, Brooks JHM, Koutedakis Y, Wyon MA. The Effect of a Comprehensive Injury Audit Program on Injury Incidence in Ballet: A 3-Year Prospective Study. Clin J Sport Med. 2013 Sep;23(5):373-8. doi: https://doi.org/10.1097/JSM.0b013e3182887f32
8. Mattiussi A, Shaw J, Williams S, Price P, Brown D, Cohen D, et al. Injury Epidemiology in Professional Ballet: A Five-season Prospective Study of 1596 Medical Attention Injuries and 543 Time-loss Injuries. Br J Sports Med [Internet]. 2021 Aug [cited 2021 May 13]; doi: http://dx.doi.org/10.1136/bjsports-2020-103817
9. Caine D, Bergeron G, Goodwin BJ, Thomas J, Caine CG, Steinfeld S, et al. A Survey of Injuries Affecting Pre-Professional Ballet Dancers. J Dance Med Sci. 2016 Aug;20(3):115-26. doi: https://doi.org/10.12678/1089-313X.20.3.115
10. Ekegren C, Quested R, Brodrick A. Injuries in Pre-Professional Ballet Dancers: Incidence, Characteristics and Consequences. J Sci Med Sport. 2014 May;17(3):271-5. doi: https://doi.org/10.1016/j.jsams.2013.07.013
11. Bowerman E, Whatman C, Harris N, Bradshaw E. A Review of the Risk Factors for Lower Extremity Overuse Injuries in Young Elite Female Ballet Dancers. J Dance Med Sci. 2015 May;19(2):51-6. doi: https://doi.org/10.12678/1089-313X.19.2.51
12. Gamboa J, Roberts L, Maring J, Fergus A. Injury Patterns in Elite Preprofessional Ballet Dancers and the Utility of Screening Programs to Identify Risk Characteristics. J Orthop Sports Phys Ther. 2008;38(3):126-36. doi: https://doi.org/10.2519/jospt.2008.2390
13. Hamilton L, Hamilton W, Warren M, Keller K, Molnar M. Factors Contributing to the Attrition Rate in Elite Ballet Students. J Dance Med Sci. 1997;1(4):131-8. Available from: https://www.ingentaconnect.com/content/jmrp/jdms/1997/00000001/00000004/art00002#expand/collapse
14. Kenny S, Whittaker J, Emery C. Risk Factors for Musculoskeletal Injury in Preprofessional Dancers: A Systematic Review. Br J Sports Med. 2016 Aug;50(16):997-1003. doi: https://doi.org/10.1136/bjsports-2015-095121
15. Rice PE, Nimphius S. When Task Constraints Delimit Movement Strategy: Implications for Isolated Joint Training in Dancers. Front Sports Act Living [Internet]. 2020 May [cited 2021 Jan 28];2. doi: https://doi.org/10.3389/fspor.2020.00049
16. Kolokythas N, Metsios GS, Galloway SM, Allen N, Wyon MA. 11+ Dance: A Neuromuscular Injury Prevention Exercise Program for Dancers. Strength Cond J [Internet]. 2022 Mar [cited 2022 May 2]; doi: https://doi.org/10.1519/SSC.0000000000000692
17. Armstrong R, Relph N. Screening Tools as a Predictor of Injury in Dance: Systematic Literature Review and Meta-analysis. Sports Med - Open. 2018 Jul 18;4(1):33. doi: https://doi.org/10.1186/s40798-018-0146-z
18. Kilburn C, Singh H, Makowski A, Musselman K. Perspectives of Physical Therapists Regarding the Use and Value of Screening Assessments and Preventative Programs for Elite-Level Dancers. J Dance Med Sci. 2020 Mar;24(1):3-11. doi: https://doi.org/10.12678/1089-313X.24.1.3
19. Mainwaring L, Finney C. Psychological Risk Factors and Outcomes of Dance Injury. J Dance Med Sci. 2017 Aug;21(3):87-96. doi: https://doi.org/10.12678/1089-313X.21.3.87
20. Moita J, Nunes A, Esteves J, Oliveira R, Xarez L. The Relationship Between Muscular Strength and Dance Injuries: A Systematic Review. Med Probl Perform Art. 2017 Mar;32(1):40-50. doi: https://doi.org/10.21091/mppa.2017.1002
21. Kolokythas N, Metsios G, Dinas P, Galloway S, Allen N, Wyon M. Growth, Maturation, and Overuse Injuries in Dance and Aesthetic Sports: a Systematic Review. Res Dance Educ. 2021 Jan;1-23. doi: https://doi.org/10.1080/14647893.2021.1874902
22. Bowerman E, Whatman C, Harris N, Bradshaw E, Karin J. Are Maturation, Growth and Lower Extremity Alignment Associated with Overuse Injury in Elite Adolescent Ballet Dancers? Phys Ther Sport. 2014 Nov;15(4):234-41. doi: https://doi.org/10.1016/j.ptsp.2013.12.014
23. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005 Dec;52(5):546-53. doi: https://doi.org/10.1111/j.1365-2648.2005.03621.x
24. Manchikanti L. Evidence-Based Medicine, Systematic Reviews,and Guidelines in Interventional Pain Management: Part 4: Observational Studies. Pain Physician. 2009 Jan 14;1;12(1;1):73-108. doi: https://doi.org/10.36076/ppj.2009/12/73
25. Buenaventura RM. Systematic Review of Therapeutic Lumbar Transforaminal Epidural Steroid Injections. Pain Physician. 2009 Jan 14;1;12(1;1):233-51. doi: https://doi.org/10.36076/ppj.2009/12/233
26. Parr AT, Diwan S, Abdi S. Lumbar interlaminar epidural injections in managing chronic low back and lower extremity pain: a systematic review. Pain Physician. 2009 Jan-Feb;12(1):163-88. doi: https://doi.org/10.36076/ppj.2009/12/163
27. Datta S, Lee M, Falco FJ, Bryce DA, Hayek SM. Systematic assessment of diagnostic accuracy and therapeutic utility of lumbar facet joint interventions. Pain Physician. 2009 Mar-Apr;12(2):437-60. doi: https://doi.org/10.36076/ppj.2009/12/437
28. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021 Mar;372:n71. doi: https://doi.org/10.1136/bmj.n71
29. Rudavsky A, Cook J, Docking S. Proximal Patellar Tendon Pathology can Develop During Adolescence in Young Ballet Dancers-A 2‐year Longitudinal Study. Scand J Med Sci Sports. 2018 Sep;28(9):2035-41. doi: https://doi.org/10.1111/sms.13095
30. Leanderson C, Leanderson J, Wykman A, Strender LE, Johansson SE, Sundquist K. Musculoskeletal injuries and generalized joint laxity in ballet dancers. (Pt. 4). [Doctoral Dissertation]. Huddinge (Stockholm): Karolinska Institutet; 2012. Available from: https://www.proquest.com/openview/b566579a33a77b3b58905f3f57e93be8/1?pq-origsite=gscholar&cbl=2026366&diss=y
31. Twitchett E, Brodrick A, Nevill. A, Koutedakis. Y, Angioi. M, Wyon. M. Does Physical Fitness Affect Injury Occurrence and Time Loss Due to Injury in Elite Vocational Ballet Students? J Dance Med Sci. 2010 Feb;14(1):26-31. [online] Available from: https://pubmed.ncbi.nlm.nih.gov/20214852/[Accessed 2022 Sep 04]
32. M, Twitchett E, Angioi M, Clarke F, Metsios G, Koutedakis Y. Time Motion and Video Analysis of Classical Ballet and Contemporary Dance Performance. Int J Sports Med. 2011 Nov;32(11):851-5. doi: https://doi.org/10.1055/s-0031-1279718
33. Liiv H, Wyon MA, Jürimäe T, Saar M, Mäestu J, Jürimäe J. Anthropometry, Somatotypes, and Aerobic Power in Ballet, Contemporary Dance, and Dancesport. Med Probl Perform Art. 2013 Dec;28(4):207-11. doi: https://doi.org/10.1055/a-1083-6539
34. Kozai A, Twitchett E, Morgan S, Wyon M. Workload Intensity and Rest Periods in Professional Ballet: Connotations for Injury. Int J Sports Med. 2020 Jun;41(06):373-9. doi: https://doi.org/10.1055/a-1083-6539
35. Krishan K, Sharma A. Estimation of Stature From Dimensions of Hands and Feet in a North Indian Population. J Forensic Leg Med. 2007 Aug;14(6):327-32. doi: https://doi.org/10.1016/j.jcfm.2006.10.008
36. Stokic E, Srdic B, Barak O. Body Mass index, body fat mass and the Occurrence of Amenorrhea in Ballet Dancers. Gynecol Endocrinol. 2005 Apr;20(4):195-9. doi: https://doi.org/10.1080/09513590400027224
37. Stracciolini A, Quinn B, Geminiani E, Kinney S, McCrystal T, Owen M, et al. Body Mass Index and Menstrual Patterns in Dancers. Clin Pediatr (Phila). 2017 Jan;56(1):49-54. doi: https://doi.org/10.1177/0009922816642202
38. Wielandt T, van den Wyngaert T, Uijttewaal J, Huyghe I, Maes M, Stassijns G. Bone Mineral Density in Adolescent Elite Ballet Dancers. J Sports Med Phys Fitness. 2019 Sep;59(9):1564-70. doi: https://doi.org/10.23736/S0022-4707.19.09700-7
39. Schmitz K, Hovell M, Nichols J, Irvin V, Keating K, Simon G, et al. A Validation Study of Early Adolescents’ Pubertal Self-Assessments. J Early Adolesc. 2004 Nov 1;24(4):357-84. doi: https://doi.org/10.1177/0272431604268531
40. Mirwald R, Baxter-Jones A, Bailey D, Beunen G. An Assessment of Maturity from Anthropometric Measurements. Med Sci Sports Exerc. 2002 May 1;34:689-94. doi: https://doi.org/10.1097/00005768-200204000-00020
41. Malina R, Choh A, Czerwinski S, Chumlea W. Validation of Maturity Offset in the Fels Longitudinal Study. Pediatr Exerc Sci. 2016 Jan;28(3):439-55. doi: https://doi.org/10.1123/pes.2015-0090
42. Khamis H, Roche A. Predicting Adult Stature Without Using Skeletal Age: The Khamis-Roche Method. Pediatrics. 1994 Oct;94(4):504-7. [online] Available from: https://europepmc.org/article/med/7936860 [Accessed 2022 Sep 04]
43. Moeskops S. The Effects of Growth, Maturation and Training on Strength and Power Development in Young Artistic Female Gymnasts [Internet] [Doctoral Dissertation]. Cardiff (Wales): Cardiff Metropolitan University; 2021. Available from: https://figshare.cardiffmet.ac.uk/articles/thesis/The_effects_of_growth_maturation_and_training_on_strength_and_power_development_in_young_artistic_female_gymnasts/14447238/1
44. Longo U, Ciuffreda M, Locher J, Maffulli N, Denaro V. Apophyseal Injuries in Children’s and Youth Sports. Br Med Bull. 2016 Dec;120(1):139-59. doi: https://doi.org/10.1093/bmb/ldw041
45. Micheli L. Preventing Youth Sports Injuries. J Phys Educ Recreat Dance. 1985;52-4. doi: https://doi.org/10.1080/07303084.1985.10603797
46. Kolokythas N, Metsios GS, Galloway S, Allen N, Wyon M. The Relationship of Year Group and Sex on Injury Incidence and Countermovement Jump in Adolescent Ballet Dancers: A Cross-Sectional Analysis. 2022 Jun 30 [online]; doi: https://doi.org/10.12678/1089-313X.091522b
47. Clarkson P, Freedson P, Skrinar M, Kelly B, Carney C. Anthropometric Measurements of Adolescent and Professional Classical Ballet Dancers. J Sports Med Phys Fitness [Internet]. 1989 Jun;29(2) [online]. Available from: https://pubmed.ncbi.nlm.nih.gov/2593653/ [Accessed 2021 Sep 28]
48. Twitchett E, Angioi M, Metsios G, Koutedakis Y, Wyon M. Body Composition and Ballet Injuries A Preliminary Study. Med Probl Perform Art. 2008 Sep 1;23. doi: https://doi.org/10.21091/mppa.2008.3020
49. Benson J, Geiger C, Eiserman P, Wardlaw G. Relationship Between Nutrient Intake, Body Mass Index, Menstrual Function, and Ballet Injury. J Am Diet Assoc. 1989 Jan;89(1):58-63. doi: https://doi.org/10.1016/S0002-8223(21)02061-7
50. Zaletel P, Sekulić D, Zenić N, Esco MR, Šajber D, Kondrič M. The Association Between Body-Built and Injury Occurrence in Pre-Professional Ballet Dancers - Separated Analysis for the Injured Body-Locations. Int J Occup Med Environ Health. 2017 Feb 21;30(1):151-9. doi: https://doi.org/10.13075/ijomeh.1896.00818
51. Frusztajer NT, Dhuper S, Warren MP, Brooks-Gunn J, Fox RP. Nutrition and the Incidence of Stress Fractures in Ballet Dancers. Am J Clin Nutr. 1990 May 1;51(5):779-83. doi: https://doi.org/10.1093/ajcn/51.5.779
52. Mountjoy M, Sundgot-Borgen JK, Burke LM, Ackerman KE, Blauwet C, Constantini N, et al. IOC Consensus Statement on Relative Energy Deficiency in Sport (RED-S): 2018 update. Br J Sports Med. 2018 Jun 1;52(11):687-97. doi: https://doi.org/10.1136/bjsports-2018-099193
53. Francisco R, Alarcão M, Narciso I. Aesthetic Sports as High-Risk Contexts for Eating Disorders-Young Elite Dancers and Gymnasts Perspectives. Span J Psychol. 2012 Mar;15(1):265-74. doi: https://doi.org/10.5209/rev_sjop.2012.v15.n1.37333
54. Lauersen J, Andersen T, Andersen L. Strength Training as Superior, Dose-Dependent and Safe Prevention of Acute and Overuse Sports Injuries: A Systematic Review, Qualitative Analysis and Meta-Analysis. Br J Sports Med. Dec 2018;52(24):1557-63. doi: https://doi.org/10.1136/bjsports-2018-099078
55. Bohannon RW. Manual Muscle Testing: Does it Meet the Standards of an Adequate Screening Test? Clin Rehabil. 2005 Sep 1;19(6):662-7. doi: https://doi.org/10.1191/0269215505cr873oa
56. Aitkens S, Lord J, Bernauer E, Fowler WM, Lieberman JS, Berck P. Relationship of Manual Muscle Testing to Objective Strength Measurements. Muscle Nerve. 1989 Mar;12(3):173-7. doi: https://doi.org/10.1002/mus.880120302
57. Escolar DM, Henricson EK, Mayhew J, Florence J, Leshner R, Patel KM, et al. Clinical Evaluator Reliability for Quantitative and Manual Muscle Testing Measures of Strength in Children. Muscle Nerve. 2001 Jun;24(6):787-93. doi: https://doi.org/10.1002/mus.1070
58. Imura A, Iino Y. Comparison of Lower Limb Kinetics During Vertical Jumps in Turnout and Neutral Foot Positions by Classical Ballet Dancers. Sports Biomech. 2017 Mar;16(1):87-101. doi: https://doi.org/10.1080/14763141.2016.1205122
59. Briggs J, McCormack M, Hakim AJ, Grahame R. Injury and Joint Hypermobility Syndrome in Ballet Dancers-a 5-Year Follow-Up. Rheumatology. 2009 Dec 1;48(12):1613-4. doi: https://doi.org/10.1093/rheumatology/kep175
60. Day H, Koutedakis Y, Wyon MA. Hypermobility and Dance: A Review. Int J Sports Med. 2011 Jul;32(7):485-9. doi: https://doi.org/10.1055/s-0031-1273690
61. Gensemer C, Burks R, Kautz S, Judge DP, Lavallee M, Norris RA. Hypermobile Ehlers-Danlos syndromes: Complex Phenotypes, Challenging Diagnoses, and Poorly Understood Causes. Dev Dyn. 2021 Mar;250(3):318-44. doi: https://doi.org/10.1002/dvdy.220
62. Ahonen J. Biomechanics of the Foot in Dance: A Literature Review. J Dance Med Sci. 2008 Aug;12(3):99-108. Available from: https://www.ingentaconnect.com/content/jmrp/jdms/2008/00000012/00000003/art00005
63. Milan K. Injury in Ballet: A Review of Relevant Topics for the Physical Therapist. J Orthop Sports Phys Ther. 1994 Feb;19(2):121-9. doi: https://doi.org/10.2519/jospt.1994.19.2.121
64. Luk P, Thordarson D, Charlton T. Evaluation and Management of Posterior Ankle Pain in Dancers. J Dance Med Sci Off Publ Int Assoc Dance Med Sci. 2013 Jun;17(2):79-83. doi: https://doi.org/10.12678/1089-313x.17.2.79
65. Kaufmann J, Nelissen R, Exner-Grave E, Gademan M. Does Forced or Compensated Turnout Lead to Musculoskeletal Injuries in Dancers? A Systematic Review on the Complexity of Causes. J Biomech. 2021 Jan;114:110084. doi: https://doi.org/10.1016/j.jbiomech.2020.110084
66. Champion L, Chatfield S. Measurement of Turnout in Dance Research A Critical Review. J Dance Med Sci. 2008 Dec;12(4):121-35. [online] Available from: https://www.ingentaconnect.com/content/jmrp/jdms/2008/00000012/00000004/art00002?crawler=true [Accessed 2022 Sep 04].
67. Russell TT. Weighing the Risks in Physical Activity. JOPERD J Phys Educ Recreat Dance. 2005 Mar;76(3):4-14. doi: https://doi.org/10.1080/07303084.2005.10608212
68. Buchheit M. The 30-15 Intermittent Fitness Test: 10 year review. Myorobie J 2010;1 [online]. Available from: https://30-15ift.com/wp-content/uploads/2013/07/buchheit-30-15ift-10-yrs-review-2000-2010.pdf [Accessed 01 June 2022].
69. Malone JJ, Barrett S, Barnes C, Twist C, Drust B. To Infinity and Beyond: The Use of GPS Devices Within the Football Codes. Sci Med Footb. 2020 Jan 2;4(1):82-4. doi: https://doi.org/10.1080/24733938.2019.1679871
70. Massard T, Carey DL, Whalan M, Sampson JA, Hulin BT, Lovell R. Comparison of Player-Dependent and Independent High-Speed Running Thresholds to Model Injury Risk in Football. J Sports Sci. 2022 Mar 19;40(6):606-13. doi: https://doi.org/10.1080/02640414.2021.2006414
Appendix
Appendix. Modified AHRQ Quality Assessment Criteria for Observational Criteria
| Area of study assessment | Focus of assessment | Reviewer mark allocation focus | Mark allocated per area | Weighted score | |
|---|---|---|---|---|---|
| Study Question | Clearly Focussed and Appropriate Question | Study Question: Title Quality (clarity of subject) | 1 | 2 | 2 |
| Study Question: Title Quality (indicate study methodology) | 1 | ||||
| Study Population | Description of Study Population | Study Population: Characteristics | 1 | 5 | 8 |
| Study Population: Gender | 1 | ||||
| Study Population: Age | 1 | ||||
| Study Population: Variability and characteristics | 2 | ||||
| Sample Size Justification | Study Population: Sample size calculations | 1 | 3 | ||
| Study Population: Explanation of sample number | 1 | ||||
| Study Population: Statistical Power | 1 | ||||
| Comparability of Subjects | Specific inclusion/exclusion criteria for all groups | COS: Mention of inclusion-exclusion criteria | 1 | 5 | 22 |
| COS: Specific population clarified | 1 | ||||
| COS: Did they volunteer or were they recruited? Was this process clearly indicated | 1 | ||||
| COS: Clarity of overall numbers of subjects included and original and adapted numbers | 1 | ||||
| COS: Inclusion exclusion criteria considered all factors | 1 | ||||
| Criteria applied equally to all groups | COS: Inclusion exclusion criteria are equal for both groups | 2 | 3 | ||
| COS: All subjects completed all screenings. | 1 | ||||
| Comparability of Groups at Baseline with disease status and prognostic factors? | COS: Injury history the same for all subjects | 1 | 3 | ||
| COS: Comp of groups in terms of injury risk exposure due to prognostic demands | 1 | ||||
| COS: Currently injured status is the same for all subjects | 1 | ||||
| Study groups comparable and non-participants in relation to confounding factors | COS: Groups comparable in age | 1 | 3 | ||
| COS: Groups comparable in gender | 1 | ||||
| COS: Groups comparable in training experience | 1 | ||||
| Did the study include a concurrent control? | COS: Control Group | 5 | 5 | ||
| Comparability of follow up for all groups at each assessment | COS: Follow up conducted over the same time frame | 1 | 3 | ||
| COS: Follow conducted by the same people | 1 | ||||
| COS: Follow up injury measure the same for all participants | 1 | ||||
| Exposure or Intervention | Clear definition of exposure | Exposure: Clear definition of the risk factors looked at | 2 | 5 | 11 |
| Exposure: Clear description of the methods of measurement | 2 | ||||
| Exposure: Clear introduction for why looking at the risk factors is necessary | 1 | ||||
| Exposure method standard, valid and reliable | Exposure: Methods standard | 1 | 3 | ||
| Exposure: Methods valid | 1 | ||||
| Exposure: Methods reliable | 1 | ||||
| Exposure measured equally in all subject groups | Exposure: Risk factor assessment at the same time for all participants | 1 | 3 | ||
| Exposure: Risk factor measurement procedure is the same for all participants | 1 | ||||
| Exposure: Risk factors were assessed the same for all participants | 1 | ||||
| Outcome Measures | Primary/Secondary Outcomes Clearly Defined | Outcome Measures: Clear definition of primary outcome and calculation steps | 2 | 5 | 20 |
| Outcome Measures: Are there any secondary measures for injury measurement clearly explained and defined in the same way | 2 | ||||
| Outcome Measures: Introduction explains the form of injury measurement | 1 | ||||
| Outcomes assessed blind to exposure or intervention | Outcome Measures: Measurement conducted by the same people that measured the risk factor | 3 | 5 | ||
| Outcome Measures: Could knowledge of the results influence the outcome measure | 2 | ||||
| Length of follow up adequate for the question? | Outcome Measures: The reason for follow up period is clearly stated | 2 | 5 | ||
| Outcome Measures: Appropriate follow up period from risk factor measurement to injury diagnosis. | 3 | ||||
| Method of the outcome, standard, valid & reliable? | Outcome Measure: Standard | 1 | 5 | ||
| Outcome Measure: Valid | 2 | ||||
| Outcome: Reliable | 2 | ||||
| Statistical Analysis | Where the statistical tests appropriate? | Statistical analysis: Missing data reported | 1 | 5 | 19 |
| Statistical analysis: Standard statistical methods used | 1 | ||||
| Statistical analysis: Do the methods chosen minimise Type 1 Error | 1 | ||||
| Statistical analysis: Do the methods chosen minimise Type 2 Error | 1 | ||||
| Statistical analysis: Are these appropriate for the number of subjects | 1 | ||||
| Multiple comparisons taken into consideration? | Statistical analysis: Could there be a multiple comparison error using the statistical methods selected | 1 | 3 | ||
| Statistical analysis: Have they used a multiple comparison test | 1 | ||||
| Statistical analysis: Was the multiple comparison test selected appropriate | 1 | ||||
| Model and Multivariate testing appropriate? | Statistical analysis: Was the statistical model/multivariate analysis described clearly | 1 | 2 | ||
| Statistical analysis: Was the statistical model or multivariate analysis chosen appropriate | 1 | ||||
| Power Calculation Provided? | Statistical analysis: Have they provided the information required to generate a power calculation | 1 | 2 | ||
| Statistical analysis: Is a power calculation and the results provided | 1 | ||||
| Assessment of Confounding | Statistical analysis: Were relationships between the variables studied investigated | 2 | 5 | ||
| Statistical analysis: Were regression models that investigated more than one factor at once used | 2 | ||||
| Statistical analysis: Were potentially confounding statistics accounted for in the analysis | 1 | ||||
| Dose-Response Assessment | Statistical analysis: Dose-response assessment used if appropriate | 2 | 2 | ||
| Results | Measure of Effect for Outcome? | Results: Measure of effect for outcome used | 1 | 5 | 8 |
| Results: Measure of effect for outcome model appropriate | 1 | ||||
| Results: Confidence intervals were provided for a measure of effect for outcome | 1 | ||||
| Results: Measure of Effect for Outcome provided a significant value | 1 | ||||
| Results: Measure of Effect for Outcomes used of significant value and CI's appropriate | 1 | ||||
| Adequacy of follow up for each study group? | Results: Follow up on the time period for the injuries reported | 1 | 3 | ||
| Results: Mean or median follow up times from risk factor measurement to injury diagnosis provided | 1 | ||||
| Results: Standard deviation and confidence intervals of injury distribution provided | 1 | ||||
| Discussion | Conclusions supported by results with potential biases and limitations are taken into consideration? | Discussion: Brief summary of results and findings | 1 | 5 | 5 |
| Discussion: Consideration and mechanisms explanation provided | 1 | ||||
| Discussion: Comparisons with other published studies provided | 1 | ||||
| Discussion: Limitations of the study provided | 1 | ||||
| Discussion: A study of the research and clinical applications of the work provided | 1 | ||||
| Funding or Sponsorship | Type and sources of support for study | Funding and Support: Mention | 2 | 5 | 5 |
| Funding and Support: Specific role of funding and support considered | 1 | ||||
| Funding and Support: Processes that the funders were involved in described | 1 | ||||
| Funding and Support: External bodies who might be influenced described | 1 | ||||
| Total Score | 100 | 100 | 100 | ||