
Musculoskeletal disorders, stress, and life quality in professors of Servicio Nacional de Aprendizaje
Desórdenes musculoesqueléticos, estrés y calidad de vida en docentes de un centro del Servicio Nacional de Aprendizaje
Noelva Eliana Montoya Grisales , Enoc Valentín González Palacio
Abstract
Objective: This research aimed to stablish the relationship between musculoskeletal disorders, stress, and quality of life of professors at a Servicio Nacional de Aprendizaje campus.
Materials and methods: The study was quantitative, non-experimental, descriptive. The sample was constituted by 55 professors, selected by a simple random sample. The instruments used were the Nordic Musculoskeletal Questionnaire, the stress questionnaire of Colombia´s Ministry of Health and Social Protection, and the Quality of Life Test, WhoQol Bref - Spanish version, authorized by the Word Health Organization. The data analysis was in SPSS-23, based on descriptive statistics (median and interquartile range) and correlative statistics (r Pearson and Rho Spearman), considering the normal distribution, which is calculated according to the Kolmogorov-Smirnov test.
Results: Positive relationship and a statistically significant association were found between musculoskeletal disorders and stress symptoms and general stress (p<0,5 and p<0,01). Negative correlation and statistical association were also found between musculoskeletal disorders and most domains of quality of life, as well as similar results when stress was related to quality of life (p <0.5 and p <0.01).
Conclusion: It was found that the greater the presence of musculoskeletal disorders and stress, the lower the quality of life in the teachers participating in the study.
Key words
Stress, Quality of life, Musculoskeletal disorders, professors, Education, Health, Pain, Distress, Risk Factors, Symptoms (source: MeSH NLM).
Resumen
Objetivo: Esta investigación se propuso establecer la relación entre los desórdenes musculoesqueléticos, el estrés y la calidad de vida de los docentes de un centro del Servicio Nacional de Aprendizaje.
Materiales y Método: El estudio fue cuantitativo, no experimental, descriptivo. La muestra estuvo constituida por 55 docentes, seleccionados de forma probabilística aleatoria simple. Los instrumentos utilizados fueron el cuestionario nórdico de desórdenes musculoesqueléticos, el cuestionario de estrés del Ministerio de la Salud y de la Protección Social y el test de calidad de vida WhoQol Bref - versión en español, autorizada por la Organización Mundial de la Salud. El análisis de datos se realizó en el software SPSS versión 23, a partir de estadísticos descriptivos (mediana y rango intercuartílico) y correlativos (r Pearson y Rho Spearman), teniendo en cuenta la distribución normal, la cual se calculó a partir de la prueba Kolmogorov Smirnov.
Resultados: Se encontró relación positiva y asociación estadísticamente significativa entre los desórdenes musculoesqueléticos y los síntomas de estrés y el estrés general (p<0,5 y p<0,01). También se encontró correlación negativa y asociación estadística entre los desórdenes musculoesqueléticos y la mayoría de dominios de la calidad de vida y resultados similares al relacionar el estrés con la calidad de vida (p<0,5 y p<0,01).
Conclusión: Se encontró que, a mayor presencia de desórdenes musculoesqueléticos y estrés, menor es la calidad de vida en los docentes participantes del estudio.
Palabras clave
Estrés, Calidad de vida, Desórdenes musculoesqueléticos, Docente, Educación, Salud, Dolor, Dificultad, Factores de riesgo, Síntomas (fuente: DeCS; BIREME).
Introduction
Work and health are an indisputable relationship in human reality; There is sufficient scientific documentation that establishes that some internal and external conditions end up affecting the life quality of employees [1-3]. These conditions, traditionally known as risk factors, are not only important from the labor or academic point of view, but also constitute a fundamental element in favor of achieving better conditions in the daily life of the employees of an institution.
In the case of the National Apprenticeship Service (SENA), this is no exception. In accordance with its Occupational Health and Safety policy, the institution implements the Occupational Health and Safety Management Subsystem (SG-SST) for the management of occupational hazard [4], in order to promote healthy environments consistent with its institutional mission. In addition, the guidelines of this subsystem are the following: “the promotion of safety and health at work as a responsibility of all employees; promoting the prevention of occupational accidents and illnesses in work environments; the identification of hazards, evaluation and assessment of risks permanently with the participation of all stakeholders in order to establish the respective controls” [4 p1]. This study is therefore part of the specific theme of social security, which, in the Colombian case, refers to certain types of occupational diseases, which have important effects on the health of people and the dynamics of organizations [1].
The Idrovo report points out [3] that among the main occupational diseases in the country are musculoskeletal disorders, which involve a series of diseases and disorders that cause pain and functional impairment of the locomotor system. The latter, in turn, creates little positive impact on the productivity of people and companies. In that sense, musculoskeletal disorders are [1] a set of problems, ailments, difficulties, and alterations of a bone, muscular, articular, tendinous, ligamentous, or nervous nature that generally arise due to inadequate positions [5], repetitive movements, conditions of the job position or activity performed or stress. On the other hand, Sahlabati et al. state [6] that this type of disorder is also a common cause of work absenteeism and accidents at work.
Another of the common diseases in the workplace, as Botero Álvarez points out, is stress, which can be defined as a mismatch between the demands of the environment and the resources available to the subject to respond to these demands [7]. This mismatch is assumed by the International Labor Organization (ILO) as a damage against which there is a physical or emotional response, which may have repercussions on the health, performance or job satisfaction of the worker [8], which it is also a regular issue in teaching, in which stress has been reported as a factor that negatively influences their health [ 9]. In fact, Salgado Roa and Leria Dulčić [10] consider that teaching is a "high risk" job to develop chronic stress, and among the most common stressful aspects the following stand out: "low salaries, scarce material and didactic resources, overcrowded classes, tension in the relationship with students, excessive workload and inexpressive participation in educational policies” [11 p26].
It is then appreciated that these mismatches, whether physical or psychological, end up generating disorders in the daily work and personal lives of workers. Faced with this, the Ministry of Labor [ 12] indicates that in the diagnostic approach for musculoskeletal disorders, in addition to including a complete physical examination, psychosocial, biomechanical, and individual risk factors are identified.
Many of these elements that are part of the work and daily life of workers are commonly addressed in the field of health and safety at work from the concept of quality of life, and traditionally attending to the perception of the subjects. In this way, quality of life is assumed “as the combination of living conditions and satisfaction based on an ordinal scale” [13].
The aspects have been approached by analyzing them individually, or in other cases they appear related to other aspects, as in the case of Rodríguez et al. [14], who associated the degree of stress with psychosocial risk factors in university teachers. For their part, Rodríguez and Dimate [15] associated musculoskeletal disorders with biomechanical risks in officials of a Colombian university. Likewise, Arango et al. [16] established, also in university employees, the relationship between musculoskeletal disorders with posture in front of a data visualization screen. A study closer to the theme of this report is that of Montoya [17], who found moderate negative correlations between stress and quality of life in a population of university employees. On the other hand, the evidence of studies that correlate musculoskeletal disorders, stress, and quality of life in common in teachers in education for work or higher education is still incipient. Therefore, this study was proposed as a general objective to establish the relationship between musculoskeletal disorders, stress, and quality of life in teachers of a center of the National Learning Service (SENA).
Based on the foregoing, the importance of this research lies primarily in two considerations: in the first instance, attend to the legal and institutional provisions, by identifying and evaluating different risk factors associated with the health of teachers, which are also aspects of great importance from the academic point of view, since they provide more evidence on their health. On the other hand, the approach to these elements is done in an integral way, by evaluating different components and establishing their relationships, thus showing how complex the study of factors associated with workers' health is, which can also generate other questions that could be addressed in further studies.
Method
Type of study
It was quantitative research, without manipulation of the independent variable (non-experimental) of a cross-sectional type and descriptive and correlative analysis.
Participants
With respect to the population surveyed, it was made up of teachers from a SENA center, which in its entirety corresponded to 105 people. Given the size of this population, a census was attempted, but this was not possible because some teachers said they did not want to participate in the study. It was then decided to take a probabilistic sample of a simple random type. The criteria for calculating the sample were the following:
Population (N): 105.
Reliability: 95% (Z=1,96).
Error (e): 5%.
p: 50%.
q: 50%.
See equations for the calculation of the sample [18]
equations for the calculation of the sample
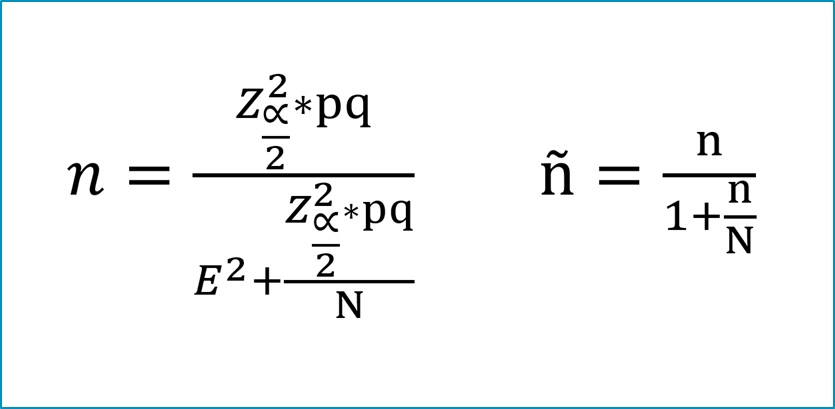
The initial sample estimate was 84.3. Since this value is greater than 10% of the population (N), a sample adjustment calculation (ñ) was performed, which determines a minimum sample of 47 subjects. In the field work, a final sample of 55 teachers was achieved, who agreed to participate voluntarily in the study, after signing the informed consent, in accordance with the provisions of resolution 008430 of the Ministry of National Health (MSN) of 1993 [ 19].
The following were established as inclusion criteria: a) be an instructor (teacher) and b) have at least twelve months working in the institution. The exclusion criteria were a) presenting a psychological illness or some musculoskeletal trauma and b) not completing any of the questionnaires partially or completely.
Instruments
One of the instruments used was the Nordic Musculoskeletal Disorders Questionnaire [20], which evaluates and quantifies, in one of its versions, the presence or absence of musculoskeletal disorders in different muscle and joint groups (neck, shoulder, elbow, wrist- hand, upper and lower back, hips-thighs, knees and ankles) in four components: presence of pain or problems (MSD) in the last twelve months, difficulties in work activities due to MSD in the last twelve months, visits to the doctor by MSD and presence of pain or problems (MSD) in the last seven days. This instrument has been validated [21] and applied [ 22] in the Colombian population. On the other hand, the questionnaire presents validity values between 80 and 100% when comparing its results with employee medical records, its test-retest reliability is greater than 77%. The questionnaire determines the presence of pain, difficulties and visits to the doctor for MSD in each area of the body, in addition to the sum of these in each of the four components that it evaluates.
The stress questionnaire of the Ministry of Health and Social Protection “is an instrument designed to assess symptoms that reveal the presence of stress reactions, divided into four main categories, according to the type of stress symptoms: a) physiological, b )social behavior, c)intellectual and labor, and d)psycho-emotional” [23 p371]. Although the validity and scales it presents are for the level of symptoms in general, the total values of the stress questionnaire when transformed range between 0 and 100 and its rating (level of stress symptoms) is as follows: very low (0-7 .8), low (7.9-12.6), medium (12.7-17.7), high (17.8-25.0) and very high (25-100). The (concurrent) validity of the questionnaire was performed with its second version [24], and calculating its correlation with the general health, vitality and mental health scales of the SF-36v2 questionnaire, significant correlations were found (p<0.01). Compared to its reliability, the Cronbach's Alpha value was 0.889.
Finally, the Quality of Life Test, WhoQol Bref -Spanish version [25], authorized by the World Health Organization in 2018, was also used. This is an instrument that assesses quality of life based on 26 questions, two of which are questions about global quality of life and general health. The response options refer to a Likert scale of five options, from which four dimensions are generated: physical health (seven items), psychological health (6 items), social relations (three items) and environment (8 items). . Each dimension can be scored from 0 to 100, or from 4 to 20 (the one used in this study), meaning that the higher the score, the better the quality of life. In a study carried out in Rionegro, Antioquia [26], the validity (convergent/divergent) and reliability of the questionnaire were analyzed, finding percentages of success in discriminant validity of 100% in all dimensions. In the convergent validity, the values of the correlations were significant and greater than 0.4. Regarding reliability, Cronbach's alpha was greater than 0.8.
Regarding the application of the instruments, to anticipate possible errors in their application and analysis, a pilot test was carried out with teachers from the institution. In the field work, the questionnaires were self-administered under the supervision and advice of one of the researchers. In the case of the stress questionnaire, we had the support of the school psychologist.
Statistical processing
Information analysis was done using SPSS version 23 software, based on descriptive parametric (standard median and deviation) and non-parametric (median and interquartile range), correlative (r Pearson and Rho Spearman) statistics. In unpaired comparisons, the student's t-test was used, taking into account the normal distribution or not of the variables, which was calculated from the Kolmogorov-Smirnov (KS) (n>50) or Shapiro-Wilk (SW) test. ) (n≤50). For the associations between the categorical variables, the Pearson contingency coefficient test was used (p<0.05).
Ethical aspects
At all times, the ethical considerations present in the Declaration of Helsinki of the World Medical Association were taken into account, as well as those established in resolution 08430 of 1993 of the National Ministry of Health [19]. Thus, this was a “risk-free” investigation, in which the privacy, dignity, and rights of the participating teachers were respected, since they agreed to participate in the study by signing an informed consent. The study was approved by the Bioethics Committee of the Universidad de San Buenaventura, Medellín.
Results
The study was carried out with 55 teachers from a SENA center. The sample consisted of 52.7% men. Regarding age, the median was 38 years (RI= 33 - 44), which reveals a group classified as young adults. Regarding the level of study, the majority of teachers have undergraduate degrees (36.4%), followed by specialization (30.9%), while only 12.7% were found at the master's level, leaving the remaining 20% of teachers with technical or technological training. As for the type of link, only 5.5% of them are holding positions in property. The rest of the sample (94.5%) has a fixed-term contract. Regarding their habits, 66.6% of them said they exercised, 90.9% did not smoke and 72.7% did not drink liquor.
Compared to the total time worked at SENA, the median was 6.17 years (RI= 3.0 - 8.3). The time worked in the Leather Design and Manufacturing Center showed a median of 3.58 years (RI= 1.3 - 8.0). 94.5% of them stated that they spent hours outside the institution on labor matters (md=10.0; RI= 5.0 - 15.0). A relevant fact was that the median time worked in front of the computer (PVD) was four hours per day (RI= 3.0 - 8.0), a habit that becomes a risk factor for suffering from some musculoskeletal disorder.
In the identification of the presence of musculoskeletal disorders, it was found that 90.1% of teachers reported having had some pain or problem in one or more areas of the body in the last twelve months, highlighting the most reported segments as the neck, lower and upper back. These same body areas were the ones that presented pain or problems in the last seven days, although in the case of this component of the Kuorinka test [20] only 69.1% of the teachers declared having presented one or more body segments with pain. Despite the presence of musculoskeletal disorders, only 47.3% of the subjects surveyed stated that this generated some type of difficulty in performing their duties at work, and only 41.8% had consulted a doctor or a specialist in health due to these types of ailments.
When relating the presence of MSD (Yes/No) in general in the last twelve months, with the variables of the social and work profile, statistically significant differences were found (p<0.05) with respect to the variable Time worked in the institution , presenting a higher prevalence (60%) teachers who have been working in the institution for less than seven years. Faced with the presence of MSD in the last seven days, there were no associations with viable sociodemographic ones. The same occurred with the association of these variables with difficulties and visits to the doctor for MSD.
Regarding stress, it was found that its total measurement presented a median of 18.56 (RI= 11.72 - 24.18), which would indicate a high stress score. In fact, in the qualitative qualification, 32.7% of the teachers presented a high level of stress, and 21.8% of them had a very high level. In 18.2% the level of stress was medium, and the remaining percentage (27.3%) corresponded to subjects with a low or very low stress rating. When associating the stress ratings (High, Medium, Low), there was no statistical association with the variables of the social or work profile (p>0.05).
In terms of quality of life, the results show a good perception of it. Psychological health stands out as the best valued (md=16.7; RI= 15.3 - 18.0), followed by physical health and social relationships. Finally, the dimension that presented the lowest score (md= 14.5; RI= 13.5 - 17.0) was the environment dimension. When comparing the assessments of the dimensions of quality of life with the variables of the social profile, it was found that, in the case of the variable (grouped) of time worked in the institution, statistically significant differences were found (p<0.05 ) in physical health. Thus, teachers who have been working for seven years or more (m=16.43; s=1.89) have a better quality of life in physical health compared to those who have been working in the institution for less time (m=1, 24, s=2.29). In psychological health, the perception was also in favor of those teachers who have been working longer (m=17.04; s=1.93), compared to those who have been working for less time (m=15.69; s=2 .60).
When comparing the dimensions of quality of life between teachers who do or do not practice physical activity, statistically significant differences (p<0.05) were found in social relationships, with this perception being better in those who do practice physical activity (m= 15.77, s=3.06), compared to those who do not (m=13.87, s=2.54). In the environment dimension, the perception was also more favorable in those who are physically active (m=15.53, s=2.19), in relation to those who stated that they did not perform any type of regular physical activity (m=14, 23, s=2.48).
When relating the musculoskeletal disorders and the different symptoms of stress and general stress (see Table 1), statistical associations were found in many of these variables. In the case of the association between the presence of musculoskeletal disorders in the last twelve months and symptoms of social behavior (r=0.277) and intellectual and labor symptoms (r= 0.310), the association was statistically significant (95%). Regarding the physiological symptoms (r= 0.398), the p value was less than 0.01, which indicates an association between the musculoskeletal disorders and the stress symptoms mentioned, that is, the greater the presence of musculoskeletal disorders presented in the last twelve months, greater are the symptoms of physiological stress, social behavior and intellectual and work. When relating general stress with musculoskeletal disorders in the last twelve months, the correlation presented is moderately positive (r=0.407) and the statistical association was also highly significant (p<0.01). No statistically significant association was found between musculoskeletal disorders in the last twelve months and psych emotional stress symptoms, although the correlation was low positive (r=0.253).
Table 1. Relationship between musculoskeletal disorders (DME) and stress symptoms
| Musculoskeletal disorders | Stress symptoms | |||||
|---|---|---|---|---|---|---|
| Physiological | Social behavior | Intellectual and labor | Psycho-emotional | General | ||
| Presence of DME last 12 months | r | 0,398** | 0,277* | 0,310* | 0,253 | 0,407** |
| Sig. | 0,003 | 0,041 | 0,021 | 0,062 | 0,002 | |
| Difficulties due to DME in the last 12 months | r | 0,341* | 0,245 | 0,269* | 0,234 | 0,354** |
| Sig. | 0,011 | 0,071 | 0,047 | 0,085 | 0,008 | |
| Visits to the doctor for DME last 12 months | r | 0,169 | 0,127 | 0,045 | 0,179 | 0,165 |
| Sig. | 0,216 | 0,354 | 0,742 | 0,191 | 0,228 | |
| Presence of DME last 7 days | r | 0,409** | 0,292* | 0,319* | 0,222 | 0,419** |
| Sig. | 0,002 | 0,03 | 0,018 | 0,104 | 0,001 | |
Note.n=55. Significant correlation **0.01 and *0.05 (bilateral).
Source: Self-made table with data from the study. Carried out with the variables of musculoskeletal disorders (MSD) and stress symptoms of the study in the month of September 2018.
In the case of relationships between difficulties at work due to musculoskeletal disorders in the last twelve months and stress, low positive correlations were found in physiological (r=0.341) and intellectual and work symptoms (r=0.269) and the general stress (r=0.3549). The statistical association between these variables was significant (p<0.05), the most relevant being the one presented with general stress (p<0.01), that is, the greater the difficulties at work due to musculoskeletal disorders in the last twelve months, the greater the physiological, intellectual and occupational stress symptoms and general stress. There was no statistically significant association with social behavioral and psycho emotional stress symptoms, although the correlation was low positive.
In the relationship between the presence of musculoskeletal disorders in the last seven days and stress, there was a low positive correlation and statistical association (p<0.05) with social behavioral stress symptoms (r=0.292) and intellectual and tasks (r=0.319). In addition, there were moderate positive correlations and a very significant association (p<0.01) with physiological symptoms (r=0.409) and general stress (r=0.419). Finally, there was no statistical association with psycho-emotional stress symptoms (see Table 1).
When relating visits to the doctor because of musculoskeletal disorders in the last twelve months with symptoms of stress and general stress, there was no correlation or statistical association between these variables, that is, consulting the doctor for musculoskeletal disorders is independent of the level of stress of the teachers.
When relating the presence of musculoskeletal disorders or pain in the last twelve months with the domains of quality of life (see Table 2), low negative correlations were found with physical (r= -0.375), psychological (r= -0.380 ) and the environment domain (r= -0.356). In social relationships, the correlation was moderately negative (rhos = -0.438). The statistical association between the dimensions of these two constructs was highly significant (p<0.01). Therefore, the greater the presence of musculoskeletal disorders (last twelve months), the lower the perception of quality of life.
Table 2. Relationship between quality of life and musculoskeletal disorders
| Life quality | Musculoskeletal disorders (MSD) | ||||
|---|---|---|---|---|---|
| Presence of DME last twelve months | Difficulties due to DME last twelve months | Visits to the doctor for DME last twelve months | Presence of DME last seven days | ||
| Physical health | r | -0,375** | -0,385** | -0,182 | -0,425** |
| Sig. | 0,005 | 0,004 | 0,183 | 0,001 | |
| Psychological | r | -0,380** | -0,434** | -0,091 | -0,410** |
| Sig. | 0,004 | 0,001 | 0,507 | 0,002 | |
| Social relationships | Rho S | -0,438** | -0,516** | -0,121 | -0,497** |
| Sig. | 0,001 | 0,000 | 0,379 | 0,000 | |
| Environment | r | -0,356** | -0,304* | -0,102 | -0,397** |
| Sig. | 0,008 | 0,024 | 0,457 | 0,003 | |
Note. n=55. Significant correlation **0.01 and *0.05 (bilateral).
Source: Self-made table with data from the study. Carried out with the variables of musculoskeletal disorders (MSD) and stress symptoms of the study in the month of September 2018.
Faced with difficulties due to musculoskeletal disorders in the last twelve months in relation to quality of life, low negative relationships were found with physical health (r= -0.385) and the environment (r= -0.304), in addition to statistically significant associations at 99 and 95%, respectively. Regarding psychological health (r= -0.434) and social relationships (r= -0.516), the correlation was moderately negative and the statistical association was highly significant (p<0.01). Therefore, the greater the difficulties due to musculoskeletal disorders, the lower the quality of life (Table 2).
In relation to the presence of musculoskeletal disorders in the last seven days, there were moderate negative correlations with physical and psychological health and social relationships (r and rhos= -0.6 to -0.4). With the environment domain, the relationship was low negative (r= 0.397) and the statistical associations were highly significant (p<0.01). Thus, the greater the presence of musculoskeletal disorders in the last seven days, the lower the quality of life. In the case of consultations for musculoskeletal disorders, there were no statistical correlations or associations with quality of life (Table 2).
When relating quality of life with stress symptoms (see table 3), physical health presented low negative correlations (r= -0.4 to -0.2) with physiological, intellectual and occupational stress symptoms and general stress, with statistically significant associations. Therefore, the greater the stress in these types of symptoms, the lower the quality of life in physical health. There was no correlation with psycho emotional stress symptoms. A very similar behavior was found in the psychological dimension of quality of life, although in relation to intellectual symptoms, the correlation was moderately negative (r= -0.417).
Tabla 3. Relationship between quality of life and stress symptoms
| Life Quality | Stress symptoms | |||||
|---|---|---|---|---|---|---|
| Physiological | Social behavior | Intellectual and labor | Psycho-emotional | General | ||
| Physical health | r | -0,280* | -0,187 | -0,269* | -0,060 | -0,285* |
| Sig. | 0,038 | 0,171 | 0,047 | 0,665 | 0,035 | |
| Psychological | r | -0,276* | -0,368** | -0,417** | -0,234 | -0,394** |
| Sig. | 0,041 | 0,006 | 0,002 | 0,085 | 0,003 | |
| Social relationships | Rho S | -0,346** | -0,426** | -0,441** | -0,341* | -0,509** |
| Sig. | 0,010 | 0,001 | 0,001 | 0,011 | 0,000 | |
| Environment | r | -0,350** | -0,480** | -0,475** | -0,296* | -0,493** |
| Sig. | 0,009 | 0,000 | 0,000 | 0,028 | 0,000 | |
Note. n=55. Significant correlation **0.01 and *0.05 (bilateral).
Source: Self-made table with data from the study. Carried out with the variables of musculoskeletal disorders (MSD) and stress symptoms of the study in the month of September 2018.
In social relationships, low negative (rhos = -0.4 to -0.2) correlations were found with physiological and psycho emotional stress symptoms and moderate negative (rhos = -0.6 to -0.4) with psychological stress symptoms. of social, intellectual and work behavior and general stress. Statistically significant associations were also presented (p<0.01), which indicates that the higher the stress, the lower the quality of life in social relationships.
Compared to the environment domain, low negative relationships (r= -0.4 to -0.2) were found with physiological and psycho emotional stress symptoms and moderate negative relationships (r= -0.6 to -0.4) with stress symptoms. of social, intellectual and work behavior and general stress, with statistically significant association (p<0.05) with psycho emotional symptoms. With the other symptoms, the statistical significance was very high (p<0.01), which generally indicates a lower quality of life in the environment domain due to work stress.
Discussion
In general, the teachers of the Leather Design and Manufacturing Center present a series of elements that are not favorable to their health. Among them, it stands out that teachers tend to spend more than four hours in front of a VDU (computer), a risk factor that was also reported in the study by Arango et al. [16], who found this same negative factor in administrative employees of a Colombian university.
A high prevalence of musculoskeletal disorders was found in the teaching population, both in the last twelve months and in the last seven days, as in other studies [6], with the neck being the most reported segment, which partially coincides with a study conducted in Chile with rural teachers [27]. There, this body segment was the one with the greatest presence, which was also reported by Cataño [5]. However, pain or problems in the elbow were also reported in the Chilean study, which differs from what was found in this study, in which the back, both upper and lower, presented a high prevalence. Unlike this study, reports of musculoskeletal pain or discomfort in the shoulders [6] and lower extremities [28 ] were also found in others. MSDs are one of the biggest disorders suffered in the work environment [29], and this is not unrelated to the teaching profession. Thus, it is essential to undertake pedagogical strategies that help mitigate this scourge in university institutions.
Regarding stress, this study, like the research by Lemos et al [2], carried out on Colombian university professors, reported high levels of stress, a situation that also occurs in university professors from different countries [7,30] and in public school teachers [31]. Regarding quality of life, professors [32] and university employees [17] tend to be satisfied. In the case of the teachers participating in this study, the results were similar. According to the above, it is possible to infer, as shown by several investigations [9,33], that the teaching profession, although satisfactory, is also a stressful job, which implies self-care in order to be aware of the well-being of others. Among the aspects associated with stress [34] are lack of control, emotional exhaustion, work overload, multiplicity of roles, job instability and lack of recognition.
In this study, a statistically significant relationship and association was found between pain and difficulties in the last twelve months and the last seven days with stress, especially in physiological, social behavior, intellectual and work symptoms and general stress, a relationship that indicates in various studies, as stated by León and Fornés [35] in their documentary review. There they report that in more than 80% of the studies analyzed (41 reports) there is a close relationship between stress variables and musculoskeletal problems.
A relationship and association was reported between musculoskeletal disorders and quality of life in physical and psychological health, social relationships, and the environment, a result similar to that reported by Agreda et al. [36], who found a relationship between the presence of musculoskeletal symptoms and the perception of quality of life in health, using the SF-36 questionnaire, although the most relevant dimensions were physical and mental health (high and moderate risk, respectively).
In the study carried out by Soto and Muñoz [37], it was reported that 92.3% of workers consider exercise to be important in the workplace and associate it as a healthy action. This makes a lot of sense to the extent that, as reported in this study, teachers who practice some type of sport or physical activity have a better perception of their quality of social life and with the environment, so that the establishment of policies and actions related to performing physical exercise in universities can be considered as a letter that helps improve the perception of quality of life in relation to health, and the mitigation of MSDs, as reported by Arango et al. [16] at a university in the city of Medellin, based on a program of active breaks.
Finally, all stress symptoms present a statistically significant association and negative correlation with the domains of social relations and environment of quality of life. The psychological health of the quality of life was related to physiological stress, social, intellectual and work behavior and general stress. In addition, the physical health of the quality of life presented negative correlations with physiological, intellectual and work stress and general stress. These results were also found in other studies [38 ,39], in which it has been reported that stress can negatively influence the quality of life in higher education professors. Similarly, Montoya [17] found negative relationships and associations between all stress symptoms and quality of life domains, but in managerial and care-level employees of a Colombian university.
Limitations and recommendations
In the first instance, it is clarified that in the results presented in this research, as they are derived from a non-experimental descriptive study, associations between variables are identified, but cause-effect relationships between them are not established. However, from this analysis other research questions and hypotheses can be derived that merit intervention processes within the institution, or organizations where the teaching function ends up diminishing the health of teachers, all with the aim of establishing programs or plans to promote health and quality of life, in addition to the implementation of actions related to the prevention of musculoskeletal disorders and stress [40].
Conclusions
In general, it was found that the greater the presence of musculoskeletal disorders and difficulties related to them, the greater the symptoms of stress in the sample investigated. With regard to quality of life, this tends to decrease with a greater presence of musculoskeletal disorders. This relationship is similar with the different stress symptoms, which tend to reduce the perception of quality of life in teachers.
In short, teachers tend to present different musculoskeletal problems and difficulties; their stress levels are mostly high and very high. Even so, their perceptions regarding the quality of life, without being perfect, is good. However, as could be seen in the results, both MSDs and stress have a negative influence on the assessments of their physical and psychological health, social relations and environment, which shows how complex the study of the health of children is. workers, in this case teachers. Therefore, the positive results derived from a study on the quality of life do not necessarily imply that there are no anomalous circumstances that are undermining it, which makes a call to continue investigating the different factors and conditioning factors that deteriorate the teaching population. or interfere with their quality of life.
references
1. Luttmann A, Jäger M, Griefahn B, Caffier G, Liebers F. Preventing Musculoskeletal Disorders in the Workplace. Berlín: World Health Organization; 2003. https://apps.who.int/iris/handle/10665/42651
2. Lemos M, Calle G, Roldán T, Valencia M, Orejuela JJ, Román-Calderón JP. Factores psicosociales asociados al estrés en profesores universitarios colombianos. Diversitas. 2019;15(1):61-72. doi: https://doi.org/10.15332/s1794-9998.2019.0001.05
3. Idrovo AJ. Estimación de la incidencia de enfermedades ocupacionales en Colombia, 1985-2000. Rev Salud Pública. 2003;5(3):263-71. doi: https://doi.org/10.1590/S0124-00642003000300003
4. Servicio Nacional de Aprendizaje. Política de salud y seguridad en el trabajo. 2016. http://compromiso.sena.edu.co/index.php?text=inicio&id=26
5. Cataño M, Echeverri MC, Penagos JC, Pérez K, Prisco JP, Restrepo P. D, et al. Riesgo biomecánico por carga estática y morbilidad sentida en docentes universitarios, Medellín 2018. Rev Ciencias la Salud. 2019;17(3):48. doi: https://doi.org/10.12804/revistas.urosario.edu.co/revsalud/a.8359
6. Sahlabadi AS, Bidel H, Rabie H, Moosavi_Kordmiri SH, Balochkhaneh FA. Relationship between the prevalence of musculoskeletal disorders and postural status and ergonomic risk factors in the workplace. Koomesh. 2021;23(4):494-501. doi: https://doi.org/10.52547/koomesh.23.4.494
7. Botero Álvarez CC. Riesgo psicosocial intralaboral y “burnout” en docentes universitarios de algunos países latinoamericanos. Cuad Adm. 2012;28(48):118-33. doi: https://doi.org/10.25100/cdea.v28i48.460
8. Organización Internacional del Trabajo. Estres en el trabajo. Ginebra: Centro Internacional de Formación de la OIT; 2016. 71 p. https://acortar.link/FAo41P
9. Cobos-Sanchiz D, López-Noguero F, Gallardo-López JA, Martín MC. Incidencia del agotamiento en los docentes universitarios: Estudio de caso en una universidad española. Form Univ. 2022;15(2):83-92. doi: https://doi.org/10.4067/S0718-50062022000200083
10. Salgado Roa JA, Leria Dulčić FJ. Síndrome de burnout y calidad de vida profesional percibida según estilos de personalidad en profesores de educación primaria. CES Psicol. 2018;11(1):69-89. doi: https://doi.org/10.21615/cesp.11.1.6
11. Corrêa Machado G, Mendes Dos Santos A, Santos Da Silva R. Teacher work: Reflections on health and teacher’s suffering. Praksis. 2020;17(1):16-30. doi: https://doi.org/10.25112/rpr.v1i0.2034
12. Ministerio de Trabajo. Recomendaciones Guía de atención integral de Seguridad y Salud en el Trabajo para desórdenes musculoesqueléticos (DME) de miembros superiores. Bogotá: Ministerio de Trabajo; 2015. https://acortar.link/ti7vTA
13. Gil-Monte PR, Cardona S. Calidad de vida laboral. En: Carrion García B, López J, Tous Pallares, editores. Promoción de la salud ocupacional. Guadalajara: AEPA; 2008. p. 75-102.
14. Rodríguez E, Sánchez-gómez J, Dorado HA, Ramírez JM. Factores de riesgo psicosocial intralaboral y grado de estrés en docentes universitarios. Rev Colomb salud Ocup. 2014;4(2):12-7. doi: https://doi.org/10.18041/2322-634X/rcso.2.2014.4908
15. Rodríguez Romero DC, Dimate García AE. Evaluación de riesgo biomecánico y percepción de desórdenes músculo esqueléticos en administrativos de una universidad Bogotá (Colombia). Investig Andin. 2015;17(31):1284-99. https://www.redalyc.org/articulo.oa?id=239040814002
16. Arango Estrada G, Adarve Restrepo KD, García Toro S, Gónzalez Palacio EV. Relación entre los desórdenes musculoesqueléticos y la postura frente a una pantalla de visualización de datos. Viref. 2017;6(1):1-12. https://acortar.link/BSs0W0
17. Montoya Marín BD. El estrés laboral y su relación con la calidad de vida de los empleados no docentes del Politécnico Colombiano Jaime Isaza Cadavid, sede Poblado, ciudad de Medellín [Tesis de Maestría en Gerencia del talento humano]. Manizales: Universidad de Manizales; 2016. https://acortar.link/3xWqDa
18. Grisales H. Muestreo en estudios descriptivos. Medellín: Facultad Nacional de Salud Púlica, Universidad de Antioquia; 2001.
19. Ministerio de Salud Nacional. Resolución número 8430 de 1993. Por la cual se establecen las normas científicas, técnicas y administrativas para la investigación en salud. Bogotá: Ministerio de Salud Nacional (Octubre 4, 1993). https://cutt.ly/yfYs1G6
20. Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233-7. doi: https://doi.org/10.1016/0003-6870(87)90010-X
21. González Palacio EV, Castro Arias E, Múnera JE, Sanmartín Velásquez M, Valencia Zuluaga NA, Valencia Gil ND. Efectos de un programa de pausas activas sobre la percepción de desórdenes músculo-esqueléticos en trabajadores de la Universidad de Antioquia | Educación Física y Deporte. Educ Física y Deport. 2011;30(1):389-399. https://acortar.link/rUA9GB
22. Castillo-Ante L, Ordoñez-Hernández C, Calvo-Soto A. Carga física, estrés y morbilidad sentida osteomuscular en trabajadores administrativos del sector público. Univ y Salud. 2020 Dec 30;22(1):17-23. doi: https://doi.org/10.22267/RUS.202201.170
23. Ministerio de Protección Social. Batería de instrumentos para la evaluación de factores de riesgo psicosocial. Bogotá: Universidad Javeriana; 2010. https://acortar.link/zBepKs
24. Villalobos G. Diseño de un sistema de vigilancia epidemiológica de factores de riesgo psicosocial en el trabajo. Cuba: Escuela Nacional de Salud Pública; 2005.
25. World Health Organization. WHOQOL-BREF : introduction, administration, scoring and generic version of the assessment: field trial version, December 1996. Geneva: WHO; 1996. https://apps.who.int/iris/handle/10665/63529
26. Cardona-Arias JA, Ospina-Franco LC, Eljadue-Alzamora AP. Validez discriminante, convergente/divergente, fiabilidad y consistencia interna del WHOQOL-BREF y el Mossf en adultos sanos de un Municipio Colombiano. Rev Fac Nac Salud Pública. 2015;33(1):50-7. https://acortar.link/eSIfXv
27. Núñez Cook S, Lizana PA. Impacto de los trastornos musculoesqueléticos en la composición corporal y calidad de vida de profesores rurales. Medwave. 2019;19(Suppl 1):117. https://acortar.link/VlyWc7
28. Almeida TEN, Ferreira REDA, Bezerra LÂ, Pereira TMDM. Analysis of the prevalence of musculoskeletal disorders and occupational stress in professors of a higher education institution in the state of Pernambuco. Rev Bras Med do Trab. 2021;18(3):274-9. doi: https://doi.org/10.47626/1679-4435-2020-542
29. Puig V. Pedagogía del dolor para la prevención de los trastornos musculoesqueléticos. Gestión práctica de riesgos laborales. 2020;(177):66-72. https://acortar.link/t8PAnD
30. Bhadana J, Saxena N, Bhatia A. Uttar Pradesh academics’ occupational stress, organisational work environment and work-life balance: A quantitative study. SA J Hum Resour Manag. 2022;20:1-8. doi: https://doi.org/10.4102/sajhrm.v20i0.1639
31. Freitas GR de, Calais SL, Cardoso HF. Estresse, ansiedade e qualidade de vida em professores: efeitos do relaxamento progressivo. Psicol Esc e Educ. 2018;22(2):319-26. doi: https://doi.org/10.1590/2175-35392018018180
32. Pereira dos Santos VL, Garcia IF, Garcia Rodrigues IC, Coelho Ribas JL, Saes Busato IM, Berté R. Estudo da qualidade de vida no trabalho de professores do ensino superior. Rev Intersaberes. 2018;11(13):187-97. doi: https://doi.org/10.22169/ri.v14i31.1419
33. Lashuel HA. Mental health in academia: What about faculty? Elife. 2020;9:9-11. doi: https://doi.org/10.7554/eLife.54551
34. Palafox Carvajal RF, Domínguez Guedea MT. Stress in university research professors: A systematic review. Salud Ment. 2021;44(5):249-56. doi: https://doi.org/10.17711/SM.0185-3325.2021.032
35. León González M, Fornés Vives J. Estrés psicológico y problemática musculoesquelética. revisión sistemática. Enferm Glob. 2015;14(2):276-300. doi: https://doi.org/10.6018/eglobal.14.2.194561
36. Agreda Moore PA, Flórez Aristizabal J, Velásquez JC. Síntomas Músculo Esqueléticos y Percepción de Calidad de Vida en Salud en trabajadores de una Curtiembre. Rev Colomb Salud Ocup. 2012;2(1):11-5. https://acortar.link/XxepxF
37. Soto Rodríguez F, Muñoz Poblete C. Percepción del beneficio del ejercicio para la prevención de trastornos musculo esqueléticos. Una perspectiva del trabajador. Cienc Trab. 2018;20(61):14-8. doi: https://doi.org/10.4067/S0718-24492018000100014
38. Gonçalves dos Santos MP, Dames da Silva KK. Níveis de estresse e qualidade de vida de professores do ensino superior. Rev Enferm da UFSM. 2017;7(4):656. doi: https://doi.org/10.5902/2179769225906
39. Paskulin M. Qualidade de vida e stress em professores de uma faculade privada [Tesis de maestría]. Campo Grande: Universidade Católica Dom Bosco; 2012.
40. Ministerio de Salud y Protección Social. Plan decenal de salu publica 2012-2021. Bogotá: Minsalud; 2012. https://acortar.link/4kTRbnv