
Effect of a virtual reality program to improve trunk stability in Paralympic shot put and javelin throwers. A case study
Efecto de un programa de realidad virtual para mejorar la estabilidad de tronco en lanzadores de bala y jabalina paralímpicos. Un estudio de casos
Luz Edith Pérez-Trejos , Lessby Gómez Salazar, Daniela Ortiz-Muñoz, Gloria-Patricia Arango-Hoyos
Abstract
Introduction: Paralympic sport originated as part of rehabilitation processes for people with disabilities. During the execution of Paralympic disciplines, motor control in the trunk region and especially in the abdomen is of great importance to prevent injuries and improve the registration of the sports record. There are many tools used by sports coaches to improve muscle strength and therefore trunk stability to reduce the risk in the sports field. However, research on the use of virtual reality along with stabilometry platforms for the training of Paralympic athletes with physical injuries are scarce.
Objective: To establish the effect of a trunk training program supported by virtual reality in high performance Paralympic athletes, shot put and javelin throwers with physical injuries who compete in throwing frames.
Materials and method: The research was designed as an intrasubject quasi-experimental study. Five high-performance Paralympic athletes with physical disabilities were evaluated. Virtual reality software that includes patterns and playful games adjustable in time and intensity and a dynamic standing platform were used as part of the intervention equipment, adjustable to the patient. This platform allows reeducating balance, proprioception, strengthening and achieving trunk control. The variables of analysis were the level of anteroposterior and lateral displacement of the trunk and changes in the volume of action. An initial evaluation, an intervention that lasted six weeks, and a final evaluation were carried out.
Results: In the initial evaluations of all athletes, a tendency towards posterior displacement was observed. In the final evaluation, the displacement ranges increase in almost all subjects except for subject 5, which showed values that remain almost stable in both the initial and final evaluations. The difference in displacement between the initial and final test on average of the participants was 6.26 degrees.
Conclusions: the positive results of trunk training supported by virtual reality for the participants constitute a contribution to the knowledge on the subject and open the possibility of including this technology in training protocols in Paralympic sports.
Keywords
Trunk stability, Paralympic throwing, virtual reality, core stability, postural balance, postural control.
Resumen
Introducción: El deporte paralímpico se originó como parte de procesos de rehabilitación para personas que tuvieran discapacidad. Durante la ejecución de las disciplinas paralímpicas el control motor en la región del tronco y en especial del abdomen es de gran importancia para prevenir lesiones y mejorar el registro de la marca deportiva. Son muchas las herramientas utilizadas por los entrenadores deportivos para mejorar la fuerza muscular y por consiguiente la estabilidad de tronco, buscando disminuir el riesgo en el ámbito deportivo. Sin embargo, las investigaciones sobre el uso de realidad virtual, junto con plataformas de estabilometría para el entrenamiento de deportistas paralímpicos con lesiones físicas, son escasos.
Objetivo: Establecer el efecto de un programa de entrenamiento del tronco apoyado en realidad virtual en deportistas de alto rendimiento paralímpicos, lanzadores de bala y jabalina con lesiones físicas y que compiten en sillas de lanzamiento.
Materiales y método: La investigación fue diseñada como un estudio cuasiexperimental intrasujeto. Se evaluaron cinco sujetos deportistas paralímpicos de alto rendimiento con discapacidad física. Se empleó un software de realidad virtual que incluye patrones y juegos lúdicos ajustables en tiempo e intensidad y una plataforma de bipedestación dinámico como parte del equipo de intervención, ajustable al paciente, que permite reeducar el equilibrio, la propiocepción, fortalecer y lograr el control del tronco. Las variables de análisis fueron el nivel del desplazamiento anteroposterior y lateral del tronco y los cambios en el volumen de acción. Se realizó una evaluación inicial, una intervención que duró de seis semanas y la evaluación final.
Resultados: En las evaluaciones iniciales de todos los atletas se observó una tendencia al desplazamiento en sentido posterior. En la evaluación final, los rangos de desplazamiento aumentan en casi todos los sujetos con excepción del sujeto 5, cuyos valores permanecen casi estables tanto en las evaluaciones iniciales como las finales. La diferencia en el desplazamiento entre la prueba inicial y final en promedio de los participantes fue de 6.26 grados.
Conclusiones: los resultados positivos del entrenamiento del tronco apoyado en realidad virtual para los participantes constituyen un aporte al conocimiento sobre el tema y abren la posibilidad de incluir esta tecnología en protocolos de entrenamiento en deporte paralímpico.
Palabras clave
Estabilidad del tronco, lanzamiento paralímpico, realidad virtual, estabilidad del core, balance postural, control postural.
Introduction
The Paralympic sport brings together people with disabilities around a high-performance sport governed by the same parameters as Olympic sport [1]. Its origins date back to the Second World War as an alternative for war veterans with spinal cord injuries [2]. The 2012 Paralympic Games brought together about 160 countries with more than 4000 athletes with different disabilities competing in 28 sports [3]. Some of those sports are track and field athletics and javelin throwing. They were adapted for the diversity of their athletes, classified according to their pathology, neurological level of injury, control, and strength of their upper limbs, lower limbs, and trunk [4] (or according to the limbs they can use). For the performance of the sport, in the case of throwers of categories F54- 57 [5], they compete in a special chair anchored to the throwing track, some with the possibility of using a support bar. Thereby, it is allowed for the athlete to use mainly the trunk and upper limbs for the sporting gesture.
In order to understand the execution of the movement in the sport of javelin throwing, it should be taken into account that, for non-disabled athletes, javelin throwing can be divided into two phases: the approach run and the delivery (also called the final push or throwing phase). The former plays a crucial role in increasing the javelin throwing velocity, an important factor in determining the throwing distance. However, in the case of athletes who use throwing frames, having little or no use of their lower limbs, the impulse transmitted to the object comes essentially from the trunk and upper limbs [6].
For the above reasons, in this type of athlete, it is significant to use and train the muscles of the so-called lumbopelvic belt or Core [7]. This has been reported by various authors [8,9], with results that are corroborated by electromyography studies that show the activity of the trunk muscles. The latter precedes the activation of the muscles of the extremities, in this case, the upper limbs, which can be interpreted as a way of creating a stable base for movement from the pelvis and spine [10]. The literature reports that patients with an injury above the mid-thoracic level, who lack volitional control of the trunk and hip musculature, may present with spinal instability. Plus, they can present an increased risk of musculoskeletal pathologies, such as low back pain, rotator cuff injuries, and other chronic health problems [11,12]. Likewise, trunk instability can cause posterior pelvic tilt (retroversion) that considerably flexes the thoracolumbar spine, leading to the appearance of kyphotic postures [13] and shortening of the lever arm of the upper extremities.
In this sense, trunk instability has an unfavorable relationship with sports injuries and several components of sports performance [14]. For example, studies report the efficacy of core stability training in athletes for managing issues such as low back pain or preventing lower limb injuries [15]. Specifically in chair throwing, Chow et al [6] state that due to adjustments to the demands of sport technique and the presence of health conditions that affect trunk stability, special emphasis should be placed on maximizing the functional potential of trunk movements in the physical preparation of Paralympic throwers, and thus optimize performance, along with injury prevention.
However, assessing and training stability is a complex task since it results from the interaction of the sensorimotor, visual, and vestibular systems [16]. Hence, the use of interactive tools with virtual environments, known as virtual reality, is becoming increasingly popular. This is a computer simulation in which graphics are used to create a realistic world, allowing real-time interactivity [17]. Virtual reality can be immersive when uses external means, such as helmets, platforms, glasses, gloves, etc. Plus, it can be non-immersive when it does not require the user to be completely focused on the program, and they can make use of a mouse or keyboard [18].
Such interventions have been successfully tested in rehabilitation processes in patients with neurological and musculoskeletal disorders, such as arthritis, cerebral palsy, and Parkinson's [19-21]. In sports, this virtual reality technology is also beginning to be widely used, especially in the field of recreation and in sports such as running, athletics, soccer, cycling, and rowing [22,23]. However, there are few reports of studies in Paralympic sports and even fewer with interventions in chair throwers.
The aim of this study is to describe the effect of an intervention based on virtual reality using the Thera-Trainer Balance platform (Thera-Trainer, Hochdorf, Germany) to improve trunk stability in a group of high performance Paralympic javelin throw athletes. The above is intended to help define its possible use in this population.
Methodology
The research was conducted as an intrasubject quasi-experimental study, evaluating the conditions of the participants before and after the intervention. The initial population was convened through the Sports Medicine Center of the Athletics League. It was constituted of seven high-achieving athletes in the Paralympic shot put and javelin, located in the functional category of F51 to F57 [5], which are those athletes who compete in throwing chairs. In these classifications, athletes have a physical disability such as spinal cord injury at different levels, amputations, or shortening of the lower extremities. Each athlete participated voluntarily and signed the informed consent form. The research has the approval of the Ethics Committee 002-018 of the Universidad del Valle, complying with the Helsinki norms.
The evaluations and interventions were performed in the movement analysis laboratory of the sports medicine unit of the Indervalle (Instituto de Deportes, Educación Física y Recreación del Valle del Cauca, by its initials in Spanish) Athletics League of Cali, Colombia. Since some athletes attended less than 80% of the virtual reality training sessions, they were excluded from the study, leaving a sample of five Paralympic athletes.
Instruments and methods
In the evaluation and intervention of trunk stability, the Thera-Trainer Balance platform (Thera-Trainer, Hochdorf, Germany) was used. It is a standing frame that can be adjusted according to the patient's needs, facilitates balance reeducation and trunk control [24,25]. In addition, it provides information on the displacement of the static and dynamic center of gravity during the tests pre-established by the equipment, using a movement sensor located on the platform. It also has a software Thera - Soft SB Basic that provides training through virtual reality, which contains recreational games that can be modified according to the needs of each athlete (Figure 1). The platform is placed at the level of the anterior iliac crest (as recommended by the manufacturer), although in cases of higher spinal injuries, the table is fixed at a level that allows the participant to achieve trunk control.
Figure 1. Thera software interface - Soft SB Basic

The evaluation protocol was standardized through one of the software tests, which consisted of moving the platform to its maximum capacity in the anterior-posterior and lateral directions for one minute. The motion sensor records the displacement information in the software in a Cartesian plane graph, allowing the evaluation of the displacement of the center of gravity during the activities. To eliminate the assistance that can be obtained from the upper limbs, the athletes were asked to cross their arms in the anterior part of the trunk to carry out the test.
A literature review was carried out to define the times, frequency, duration of the sessions, and type of exercises. The following intervention protocol was determined: six weeks, three weekly sessions of 45 minutes each [26,27]. All the exercises included in the Thera soft software were used. The mechanical resistance of the platform was adjusted to 50% for the initial evaluations and was increased as the interventions progressed.
Initial evaluations were also carried out, consisting of three repetitions of each given activity, to favor the learning effect and the interaction with the software. Thus, the baseline was established to carry out a final evaluation. The software generates the results in a PDF. The document shows a report with the graphs of the displacements can be evidenced to analyze them later very descriptively, according to the differences in the graphical records of the initial and final evaluations.
As an additional variable, each athlete was evaluated for trunk stability before and after the intervention, based on the volume of action in sedentary position. [28]. This evaluates the maximum displacement of the trunk in the anterior-posterior and lateral direction in a chair without backrest, and is used as a functional reference in Paralympic sport [29]. Although the scale has qualitative assessment parameters (Table 1), trunk displacement was also measured in degrees based on videography for this study.
Table 1. Rating scale of the Volume of Action, according to the IWBF [30].
| IWBF classification based on function | |
|---|---|
| Clasificación | Function |
| 1.0 |
• Little or no controlled movement of the trunk in the frontal plane • Balance in the frontal and lateral directions is significantly affected • Players need their arms to return to the upright (initial) position |
| 2.0 |
• Partially controlled trunk movement in the frontal plane • No controlled movement of the trunk in the lateral plane |
| 3.0 |
• Good trunk movement in the frontal plane • No controlled movement of the trunk in the lateral plane |
| 4.0 |
• Normal trunk movements, but usually the player has difficulty with controlled movement to one side |
| 4.5 |
• Normal trunk movements in all directions • Able to tilt the trunk to one side or the other without limitations |
Note: There are situations where a player does not seem to fit perfectly in one class, presenting characteristics of two or more classes. In this case, the classifier may attribute the player a rating of half a point, 1.5, 2.5 or 3.5. This is generally done only when the player cannot be assigned a defined class, and should not be considered as the first choice for the classifier.
Results
After applying the inclusion and exclusion criteria, the population analyzed consisted of five high-achieving athletes from the Valle National Team, Colombia, who participated in the Paralympic javelin throw. Three athletes present a history of spinal trauma; the other two have lower limb affectations. The demographic and clinical characteristics of the athletes participating in the study are presented below (Table 2).
Table 2. Demographic and clinical characteristics of the athletes
| Subjects | Age (years) | Genre | Mechanism of injury | Injury sequelae | Time of evolution (years) | Medical functional classification |
|---|---|---|---|---|---|---|
| Subject 1 | 47 | Male | Traumatic accident | T4 Spinal Trauma | 10 | F54 |
| Subject 2 | 33 | Male | Traffic accident | Spinal cord trauma T4 | 10 | F54 |
| Subject 3 | 35 | Female | Traffic accident | T11 Spinal cord trauma | 8 | F55 |
| Subject 4 | 25 | Female | Congenital pathology | Femur shortening 10 cm | 25 | F57 |
| Subject 5 | 45 | Male | Traumatic accident | Transtibial amputation | 38 | F57 |
As mentioned previously in this paper, the subjects were evaluated before and after the intervention sessions on the stabilometric platform (Figure 2). The software automatically produces graphical results that allow the analysis of the data obtained during the sessions (Figure 3). Subsequently, the final results were plotted according to the maximum displacement achieved by each athlete, both in the lateral and anteroposterior direction, and the average displacement value to identify the tendency to move in a particular direction (Figures 4 and 5).
Figure 2. Training images with Thera-Trainer Balance

Figure 3. Scaled Paralympic evaluations.
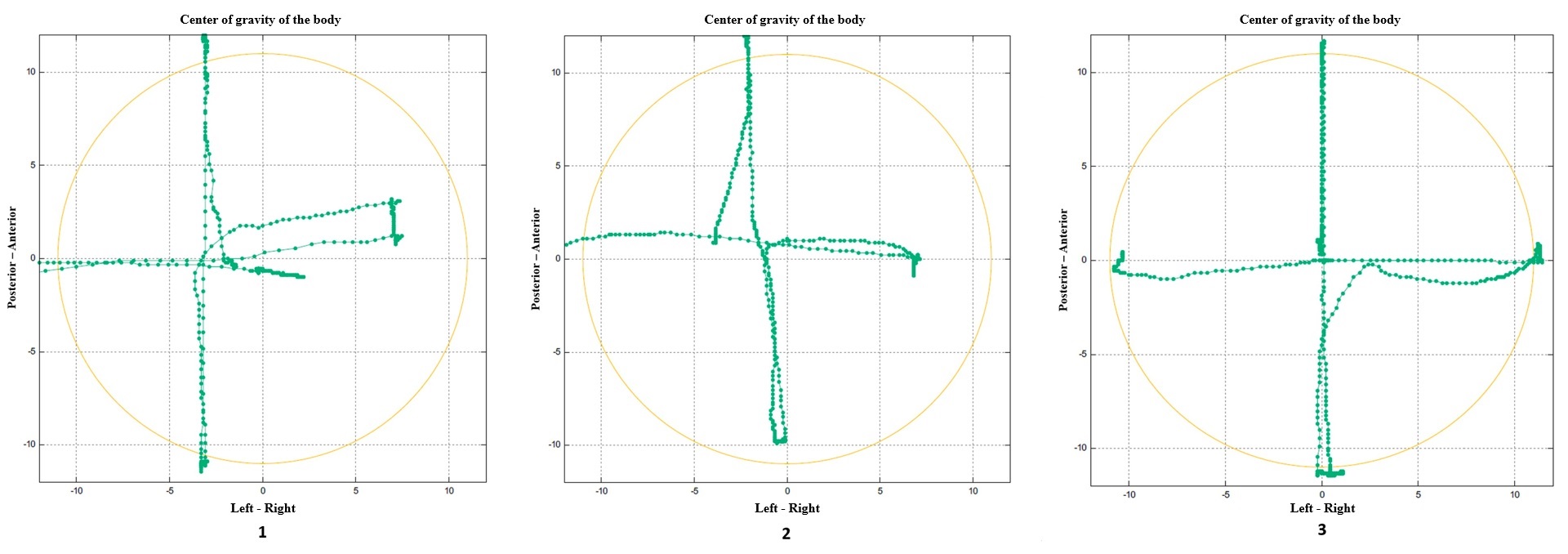
Figure 4. Lateral (right-left) displacement of the CG before and after the intervention
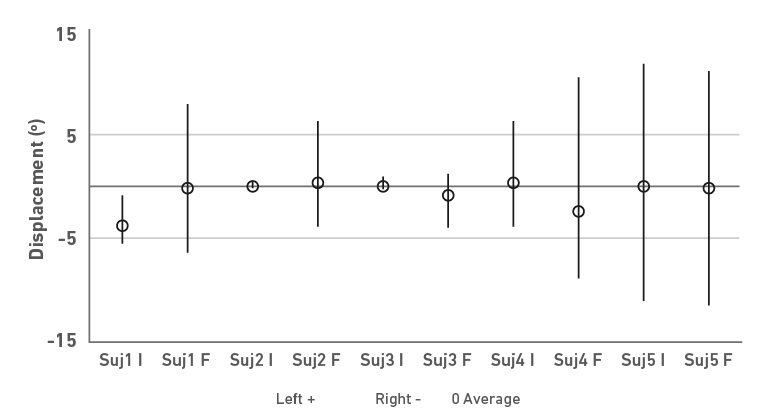
Figure 5. Anteroposterior displacement of the CG before and after the intervention
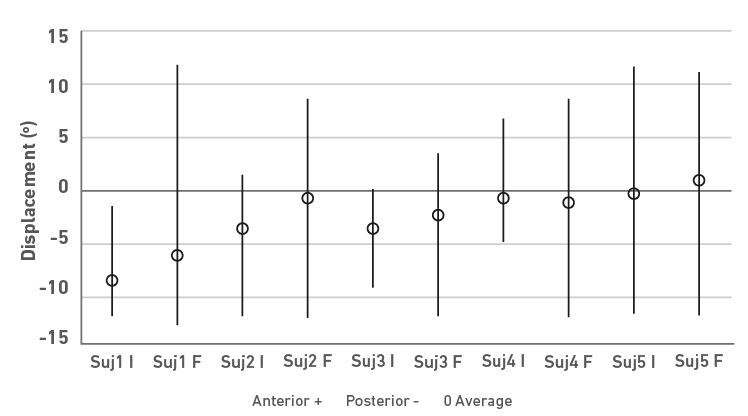
In the initial tests, it is possible to observe a smaller displacement range in the athletes without spinal cord injury (subjects 4 and 5) compared to the other athletes. However, there is more incredible difficulty in displacing the center of gravity (CG) laterally than in the anterior-posterior direction. In all of them, there is a tendency to move in the posterior direction.
In the final evaluation, the range of displacement increases in almost all subjects (Table 3), except for subject 5, whose values remain practically stable in both the initial and final evaluations. The difference in displacement between the initial and final test on average of the participants was 6.26 degrees. Subjects 2 and 4 presented the greatest changes in the right-left direction, and subjects 1 and 4 in the anterior-posterior direction.
Table 3. Total displacement values and differences between initial and final evaluations
| Subject | Test | Right-left shift | Antero-posterior displacement | ||||
|---|---|---|---|---|---|---|---|
| Total* (degrees) | Difference Initial-Final | Average | Total* (degrees) | Difference Initial-Final | Average | ||
| 1 | Initial | 6.13 | 8.20 | 6.26 | 13.25 | 11.12 | 6.78 |
| Final | 14.33 | 24.37 | |||||
| 2 | Initial | 0.47 | 9.69 | 12.87 | 7.57 | ||
| Final | 10.16 | 20.44 | |||||
| 3 | Initial | 1.01 | 4.11 | 8.99 | 6.06 | ||
| Final | 5.11 | 15.04 | |||||
| 4 | Initial | 9.86 | 9.25 | 11.38 | 8.82 | ||
| Final | 19.11 | 20.21 | |||||
| 5 | Initial | 21.46 | 0.06 | 21.66 | 0.34 | ||
| Final | 21.52 | 22.00 | |||||
Note: * Total displacement magnitude values, regardless of its direction.
Concerning trunk control measured through the volume of action, the changes were less evident in quantitative terms. There was no significant variation in the results evaluated from the initial and final assessment, since subjects 4 and 5 maintained the maximum score of the rating scale. In contrast, in subjects 1, 2 and 3, who present spinal cord injury, the final qualitative assessment increased its value concerning the initial one. Only subject three presented changes in the degrees of trunk displacement in flexion and lateral inclinations (Table 4).
Table 4. Changes in the volume of action before and after the intervention.
| Volume of Action | ||||||||
|---|---|---|---|---|---|---|---|---|
| Athlete | Flexion | Extension | Lateral inclinations | IWBF Classification | ||||
| Initial | Final | Initial | Final | Initial | Final | Initial | Final | |
| Sujeto 1 | 20° | 20° | 20° | 20° | 20° | 20° | 1.5 | 2.5 |
| Sujeto 2 | 20° | 20° | 20° | 20° | 20° | 20° | 1.0 | 2.0 |
| Sujeto 3 | 20° | 40° | 40° | 40° | 40° | 60° | 3.0 | 4.0 |
| Sujeto 4 | 60° | 60° | 60° | 60° | 60° | 60° | 4.5 | 4.5 |
| Sujeto 5 | 60° | 60° | 60° | 60° | 60° | 60° | 4.5 | 4.5 |
Discussion
The role of trunk stability in sports performance is controversial because little is known about its direct relationship. However, numerous researchers consider that adequate trunk stability prevents injuries and enables better sports performance, being more evident in some sports disciplines, such as throwing [31,32]. Hence, coaches have to always look for the best strategies to achieve the highest possible level of stability in this body segment.
In the initial assessments carried out on the five Paralympic athletes, four of them showed deficiencies in trunk control, and only one completed the range of motion required by the platform, even though the level of demand of the test was adjusted for all of them at 50% of the maximum resistance offered by the Thera Trainer Balance. As expected, the athletes with spinal cord injury obtained the lowest results. Yet, the athlete who had problems with the shortening of a limb had difficulty completing the test.
In people with thoracic spinal cord injury, depending on the level of damage, motor control of some or all trunk muscles is affected, which may result in the inability or difficulty to sit without support, stand, walk or make transitions of movement [33]. In athletes 1, 2 and 3 of this research, not only is there a history of traumatic spinal cord injury but there is also a long time of evolution of the pathology-more than eight years- This led to think that the changes in postural control after the development of the proposed exercise program would be minimal. However, significant improvements in trunk displacement were evidenced in these three subjects, which can be explained by the existence of neuromuscular plasticity that allows individuals with spinal cord injury to generate new muscular synergies when the patient is subjected to repetitive multidirectional training [34]. In addition to the aforementioned results, the athletes stated that the best effect for them was the ability to stand during the sessions and the decrease in spasticity and clonus associated with their pathology.
As previously mentioned, athlete 4, who presented a lower limb shortening, showed difficulties in performing trunk movement, especially in the lateral direction. This may suggest that beyond physical limitations that directly affect the spine-as in the case of spinal cord injury-other factors can generate poor muscle balance, such as overuse fatigue, history of muscle or joint injury, lack or imbalances in muscle strength due to disuse or inadequate training techniques, among others [35]. These factors should be considered within the assessment and monitoring of the physical condition of athletes. At the end of the training sessions, athlete 4 improved her performance without reaching the maximum value in the test. During the execution of the virtual activities, each athlete had to overcome a resistance generated by the platform, leading to fiber recruitment and Core muscle activation, which may explain the improvement in trunk stability reflected in the displacements recorded by the software [31].
On the other hand, concerning the data obtained, a tendency towards trunk extension was observed in all the participants, although this was more evident in the athletes with spinal cord injury. Even though the lack of abdominal strength can explain this to bring the trunk forward, the design of the standing platform makes it easier for the subjects to drop the body backward without the participation of the trunk extensor muscles.
In relation to the training methods to improve trunk stability, it is considered that these should include strategies both to train cognitively and to improve the sensory input of the trunk musculature [36]. In addition, other aspects that may directly influence athletic performance, such as each athlete's social, emotional and clinical aspects, should be taken into account [37]. In the case of the use of a standing platform supported by virtual reality, it has been demonstrated that it can generate good results for the intervened athletes due to the demand imposed by the bipedal posture, the variety of exercises that integrate range of motion, reaction speed and precision, as well as the possibility of graduating the level of complexity in an individualized manner. All this results in a highly demanding and motivating activity for its execution.
Although Vera-Garcia [38] mentions that there is no clarity on the frequency and intensity of the exercise sessions for trunk stability work, the structure of three weekly sessions of half an hour for six weeks, chosen for this research, seems to generate good results. However, given the small sample of participants, it is necessary to extend the intervention to more subjects to validate the evidence.
The transfer of stability-enhancing training to activities of daily living or sports is a controversial topic [39]. In the case of this research, the evaluation of the volume of action was intended to have an approach to the conditions of when using a throwing frame. As observed, the gain in the range of motion on the platform did not necessarily transfer to the action volume. However, the qualitative classification did improve in some athletes.
Conclusions
The results showed the positive effect of training supported by virtual reality for trunk stability of the participants in this research, in addition to obtaining other benefits through standing, such as reducing some alterations associated with their pathology. The research constitutes an important contribution to the knowledge on the subject. It also opens the possibility of including this technology as part of the training protocols in this population.
Highlights:
• The results demonstrate the possibility of using stability platforms and virtual reality software to improve trunk motor control.
• The stabilometric platform can be considered a good tool for intervention in patients with spinal cord injury.
• The use of virtual reality and stability platforms could be included as part of regular training for athletes with disabilities and other similar populations.
References
1. Ruiz S. Deporte paralímpico: una mirada hacia el futuro. Revista UDCA Actualidad & Divulgación Científica. 2012;15:97-104. doi: https://doi.org/10.31910/rudca.v15.nsup.2012.897
2. Legg D. Paralympic Games: History and Legacy of a Global Movement. Physical Medicine and Rehabilitation Clinics of North America [Internet]. 2018 May 1;29(2):417-25. doi: https://doi.org/10.1016/j.pmr.2018.01.008
3. Morriën F, Taylor MJD, Hettinga FJ. Biomechanics in Paralympics: Implications for Performance. International Journal of Sports Physiology and Performance [Internet]. 2017 May 1;12(5):578-89. Doi: https://doi.org/10.1123/ijspp.2016-0199
4. Reina R, Vilanova-períz N. Guía sobre clasificación de la discapacidad en deporte paralímpico. En: Limencop SL, editor. España; 2016. p. 31-37.
5. Moya Cuevas RM. Deporte adaptado. España: Ceapat-Imserso; 2014 Sep 14. Disponible en: http://riberdis.cedid.es/handle/11181/5025
6. Chow JW, Kuenster AF, Lim Y tae. Kinematic analysis of javelin throw performed by wheelchair athletes of different functional classes. J Sports Sci Med. 2003;2(2):36. Disponible en: http://www.ncbi.nlm.nih.gov/pmc/articles/pmc3938047/
7. Wirth K, Hartmann H, Mickel C, Szilvas E, Keiner M, Sander A. Core Stability in Athletes: A Critical Analysis of Current Guidelines. Sports Medicine. 2016 Jul 30;47(3):401-14. doi: https://doi.org/10.1007/s40279-016-0597-7
8. Ghasempoor KH, Rahnama N, Bagherian S, Wikstrom EA. P18 The effect of core stability training on functional movement patterns in collegiate athletes. BMJ Publishing Group Ltd and British Association of Sport and Exercise Medicine; 2017. doi: https://doi.org/10.1136/bjsports-2017-anklesymp.50
9. Manchado C, García-Ruiz J, Cortell-Tormo JM, Tortosa-Martínez J. Effect of core training on male handball players’ throwing velocity. J Hum Kinet. 2017;56(1):177-85. doi: https://doi.org/10.1515/hukin-2017-0035
10. Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in neuromuscular control of the trunk predict knee injury risk: prospective biomechanical-epidemiologic study. Am J Sports Med. 2007;35(7):1123-30. doi: https://doi.org/10.1177/0363546507301585
11. Lema CPH, Parra JEP. Lesiones medulares y discapacidad: revisión bibliográfica. Aquichan. 2010;10(2):157-72. doi: https://doi.org/10.5294/aqui.2010.10.2.5
12. Bjerkefors A, Squair JW, Chua R, Lam T, Chen Z, Carpenter MG. Assessment of abdominal muscle function in individuals with motor-complete spinal cord injury above T6 in response to transcranial magnetic stimulation. J Rehabil Med. 2015;47(2):138-46. doi: https://doi.org/10.2340/16501977-1901
13. Triolo RJ, Bailey SN, Lombardo LM, Miller ME, Foglyano K, Audu ML. Effects of intramuscular trunk stimulation on manual wheelchair propulsion mechanics in 6 subjects with spinal cord injury. Arch Phys Med Rehabil. 2013;94(10):1997-2005. doi: https://doi.org/10.1016/j.apmr.2013.04.010
14. Hides JA, Stanton WR. Can motor control training lower the risk of injury for professional football players? Medicine & Science in Sports & Exercise. 2014;46(4):762-8. doi: https://doi.org/10.1249/MSS.0000000000000169
15. De Blaiser C, Roosen P, Willems T, Danneels L, Bossche L Vanden, De Ridder R. Is core stability a risk factor for lower extremity injuries in an athletic population? A systematic review. Physical therapy in sport. 2018;30:48-56. doi: https://doi.org/10.1016/j.ptsp.2017.08.076
16. Nesser TW, Lee WL. The relationship between core strength and performance in division i female soccer players. J Exerc Physiol Online. 2009;12(2):1750-4. doi: https://doi.org/10.1519/JSC.0b013e3181874564
17. Martínez FJP. Presente y Futuro de la Tecnología de la Realidad Virtual. Creatividad y sociedad. 2011;16:1-39. Disponible en: https://pdfslide.tips/technology/presente-y-futuro-de-la-tecnologia-de-la-realidad-virtual.html?page=1
18. Aznar Díaz I, Romero-Rodríguez JM, Rodríguez-García AM. La tecnología móvil de Realidad Virtual en educación: una revisión del estado de la literatura científica en España. EDMEDTIC 2018;7(1):256-274. doi: https://doi.org/10.21071/edmetic.v7i1.10139
19. Shahmoradi L, Almasi S, Ahmadi H, Bashiri A, Azadi T, Mirbagherie A, et al. Virtual reality games for rehabilitation of upper extremities in stroke patients. Journal of Bodywork and Movement Therapies. 2021 Apr 1;26:113-22. doi: https://doi.org/10.1016/j.jbmt.2020.10.006
20. Choi YH, Paik NJ. Mobile Game-based Virtual Reality Program for Upper Extremity Stroke Rehabilitation. J Vis Exp [Internet]. 2018 Mar 8;2018(133). doi: https://doi.org/10.3791/56241
21. Feng H, Li C, Liu J, Wang L, Ma J, Li G, et al. Virtual Reality Rehabilitation Versus Conventional Physical Therapy for Improving Balance and Gait in Parkinson’s Disease Patients: A Randomized Controlled Trial. Medical Science Monitor: International Medical Journal of Experimental and Clinical Research [Internet]. 2019;25:4186. doi: https://doi.org/10.12659/MSM.916455
22. Neumann DL, Moffitt RL, Thomas PR, Loveday K, Watling DP, Lombard CL, et al. A systematic review of the application of interactive virtual reality to sport. Virtual Reality. 2018;22(3):183-98. doi: https://doi.org/10.1007/s10055-017-0320-5
23. de Araújo AVL, Neiva JFDO, Monteiro CBDM, Magalhães FH. Efficacy of Virtual Reality Rehabilitation after Spinal Cord Injury: A Systematic Review. BioMed Research International. 2019;. doi: https://doi.org/10.1155/2019/7106951
24. Fasola J, Kannape OA, Bouri M, Bleuler H, Blanke O. Error Augmentation Improves Visuomotor Adaptation during a Full-Body Balance Task. In: 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC). IEEE; 2019;1529-33. doi: https://doi.org/10.1109/embc.2019.8857523
25. Chisholm DH, Ferrer BC, Domínguez NMC, Fuentes YP, Perdomo VC, Castillo YS. Protocolo de actuación de los equipos Thera Trainer en trastornos de equilibrio, postura y marcha del adulto mayor. Revista Cubana de Medicina Física y Rehabilitación. 2017;9(1):1-14. Disponible en: https://www.medigraphic.com/cgi-bin/new/resumen.cgi?IDARTICULO=75117
26. Killane I, Fearon C, Newman L, McDonnell C, Waechter SM, Sons K, et al. Dual motor-cognitive virtual reality training impacts dual-task performance in freezing of gait. IEEE J Biomed Health Inform. 2015;19(6):1855-61. doi: https://doi.org/10.1109/JBHI.2015.2479625
27. Peruzzi A, Cereatti A, Della Croce U, Mirelman A. Effects of a virtual reality and treadmill training on gait of subjects with multiple sclerosis: a pilot study. Mult Scler Relat Disord. 2016;5:91-6. doi: https://doi.org/10.1016/j.msard.2015.11.002
28. Commission IPC. A Guide to the IWBF Functional Classification System for Wheelchair Basketball Players. Ontario: International Paralympic Committee ; 2004.
29. Gustavo de Souza Pena L, Barra Danyau C, Fernández M, Gustavo Teixeira Fabrício dos Santos L, Paulo Casteleti de Souza J, Luarte Rocha C, et al. Limitaciones y Posibilidades en el Entrenamiento del Baloncesto en Silla de Ruedas. Revista Peruana de ciencia de la actividad fisica y del deporte [Internet]. 2020 Jun 14 [cited 2022 Aug 18];7(4):9-9. Disponible en: https://rpcafd.com/index.php/rpcafd/article/view/117/163
30. de Souza Pena LG, Danyau CB, Fernández M, dos Santos LGTF, Casteletti JP, Rocha CL, et al. Limitaciones y Posibilidades en el Entrenamiento del Baloncesto en Silla de Ruedas. Revista Peruana de ciencia de la actividad fisica y del deporte. 2020;7(4):9. Disponible en: https://rpcafd.com/index.php/rpcafd/article/view/117
31. Reed CA, Ford KR, Myer GD, Hewett TE. The effects of isolated and integrated ‘core stability’ training on athletic performance measures. Sports medicine. 2012;42(8):697-706. doi: https://doi.org/10.1007/BF03262289
32. Saeterbakken AH, Van den Tillaar R, Seiler S. Effect of core stability training on throwing velocity in female handball players. The Journal of Strength & Conditioning Research. 2011;25(3):712-8. doi: https://doi.org/10.1519/jsc.0b013e3181cc227e
33. Harvey L. Management of Spinal Cord Injuries E-Book: A Guide for Physiotherapists. Amsterdam: Elsevier Health Sciences; 2008.
34. Milosevic M, Yokoyama H, Grangeon M, Masani K, Popovic MR, Nakazawa K, et al. Muscle synergies reveal impaired trunk muscle coordination strategies in individuals with thoracic spinal cord injury. Journal of Electromyography and Kinesiology. 2017;36:40-8. doi: https://doi.org/10.1016/j.jelekin.2017.06.007
35. Larson DJ, Brown SHM. The effects of trunk extensor and abdominal muscle fatigue on postural control and trunk proprioception in young, healthy individuals. Hum Mov Sci. 2018;57:13-20. doi: https://doi.org/10.1016/j.humov.2017.10.019
36. Zazulak B, Cholewicki J, Reeves PN. Neuromuscular control of trunk stability: clinical implications for sports injury prevention. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2008;16(8):497-505. doi: https://doi.org/10.5435/00124635-200809000-00002
37. Rojas A, Fernando J. Entrenamiento en alto rendimiento deportivo: desde las percepciones de los atletas paralímpicos [Trabajo de grado]. Bogotá: Universidad Pedagógica Nacional; 2019.
38. Vera-García FJ, Barbado D, Moreno-Pérez V, Hernández-Sánchez S, Juan-Recio C, Elvira JLL. Core stability: evaluación y criterios para su entrenamiento. Rev Andal Med Deport. 2015;8(3):130-7. doi: https://doi.org/10.1016/j.ramd.2014.02.005
39. Anderson K, Behm DG. The impact of instability resistance training on balance and stability. Sports medicine. 2005;35(1):43-53. doi: https://doi.org/10.2165/00007256-200535010-00004